|
I. Disorientation/Lightheadedness
Possible causes: A dental patient who presents with disorientation may be suffering a serious medical problem. Medical problems potentially accounting for disorientation/lightheadedness include both acute-onset and chronic medical conditions. Acute onset conditions include stroke, transient ischemic attack (TIA), acute cardiac arrhythmia, hypo or hyperglycemia secondary to poor diabetes control, seizure, trauma, cerebral infection, complicated migraine or electrolyte imbalance. Chronic conditions that could cause lightheadedness or disorientation include degenerative brain disease (Alzheimer’s disease) or neurological neoplasm as well as other conditions too numerous to review here. The following review will discuss the management of cardiovascular conditions that could predispose a patient to develop acute-onset disorientation/lightheadedness. Once the dentist recognizes that a patient is suffering from this symptom, a review of the medical history may provide clues as to the relationship of this symptom to underlying medical disease if any. The following cardiovascular conditions are reviewed as they relate to this symptom and the measures that the dentist should consider when managing a patient of this type.
Stroke:
Cause: It should be emphasized that acute-onset disorientation/lightheadedness carries a higher level of concern for the patient and dentist. The primary problem with acute-onset disorientation/lightheadness is that it may result from a stroke. More common symptoms associated with stroke include loss of motor function, inability to speak or loss of consciousness. However, the dentist must be cognizant of the possibility of stroke in subjects without these more common symptoms.
Assessment: A quick screening for stroke (Cincinnati Prehospital Stroke Scale) that can be administered in less than one minute includes an assessment of facial droop (paralysis), arm drift when the patient closes their eyes and extends both arms straight out in front and difficulty in speaking (ask the patient to say "you can’t teach an old dog new tricks"). If the patient shows facial droop or is positive for arm drift or difficulty with speaking, there is a 72% chance that an ischemic stroke has occurred. If all three features are evident, the risk of stroke increases to 85%2.
Management: If there is likelihood that a stroke has occurred, medical evaluation should occur quickly. For fibrinolytic therapy (Alteplase, [tissue plasminogen activator, tPA, Tenecteplase or Reteplase]) to be effective, therapy should begin within three hours following the onset of symptoms of an ischemic stroke2. For a patient to be eligible for fibrinolytic therapy, an emergency facility must verify by noncontrast CAT scan that the stroke is not hemorrhagic. Therefore, if a stroke is suspected, transport to a suitably equiped medical emergency facility should occur immediately so that necessary diagnostic work can be completed within three hours since the onset of signs or symptoms of a stroke. If the stroke management facilities at a local hospital are not certain, the dentist should seek immediate advice from a local emergency room for referral to a suitable stroke management medical center.
Transient Ischemic Attack:
Cause: Transient ischemic attack is similar to a stroke except that permanent damage to the brain typically does not occur and as the name implies, the stroke-like effects are transient.
Management: Management of a patient with a TIA is essentially the same as that for a stroke (immediate transport to an emergency medical facility). An additional consideration for a patient with a recent history of TIA is that the risk for subsequent stroke is greatest during the weeks that follow a TIA.
Atherosclerosis:
Cause: Arterial stenosis secondary to atherosclerosis of the major arteries of the neck may also cause lightheadedness, but this condition is more likely to affect motor function or eyesight and is more likely to be manifest with exertion rather than at rest. Restricted blood flow through one or both carotid arteries may produce altered cerebral function due to decreased delivery of oxygenated blood to the brain. Restricted blood flow through coronary arteries due to atherosclerosis is associated with myocardial ischemia and chest pain (See below).
Assessment: Review the medical history for indicators of ischemic disease including a prior physical examination evauating for bruits in the major arteries, particularly the carotid arteries, indicating significant arterial stenosis (narrowing of the artery lumen).
Management: Documented arterial occlusion/s in a symptomatic patient carries a higher risk for stroke. Referral for outpatient medical evaluation (non-emergency, medical evaluation) should occur promptly if the patient indicates a recent episode of disorientation/lightheadedness.
Additional Considerations: Disorientation/lightheadedness due to a stroke may produce dementia (reduced cognitive function). However, dementia in most dental patients is of long duration and the underlying brain disease most frequently associated with dementia is Alzheimer’s disease. If a patient cannot remember simple information, the dentist should consider the possibility of dementia and refer the patient to a physician for further evaluation. Stroke or TIA requires immediate emergency medical attention. Atherosclerosis and dementia of a slow progressive time course suggest medical referral and perhaps delay or modification of dental treatment. The dentist is not expected to diagnose stroke or TIA nor to distinguish these conditions from atherosclerotic dementia or Alzheimer’s disease. Therefore, medical consultation is essential in these cases.
Abnormal Cardiac Rhythm:
Cause: Disorientation/lightheadedness may also be caused by an abnormal cardiac rhythm.
Assessment: If a prior history of abnomal cardiac rhythm is not listed in the dental record, the cardiac rhythm can be detected by palpating the radial pulse. Cardiac arrhythmias include changes in the heart rate (fast is a tachycardia and slow is a bradycardia) or changes in the rhythm of the heartbeat (irregular rhythms). The irregular heart rate can be detected by palpating for a change in rhythm and/or pulse strength at the radial artery. Irregular heart beats can originate from the atria or the ventricles. Ventricular premature beats typically reveal a considerably stronger pulse that occurs approximately one half beat early. Patients are often aware of these pre-systolic beats but accompanying symptoms may not exist, suggesting that the condition does not requires immediate medical attention.
Management: If an abnormal cardiac rhythm exists in combination with decreased cognition or lightheadedness, the symptoms suggests that the altered cardiac rhythm is impairing blood flow to the cerebral cortex (the patient is hemodynamically unstable). In this case, the patient should be transported to a medical facility for immediate treatment. Examples of rhythms that can result in lightheadedness include atrial fibrillation/flutter, ventricular tachycardias or bradycardia. Other common abnormal cardiac rhythms in dental patients that may or may not be symptomatic include premature ventricular contractions (PVCs), heart block, or regularly irregular cardiac rhythms including irregularly occurring bigemini or trigemini. At the very least, a dental patient with a history of cardiac disrhythm and presenting symptoms (disorientation/lightheadedness) should have continuous blood pressure monitoring and receive supplemental oxygen either by nasal cannula or by face mask (deliver oxygen at 4-6 liters/minute). Concern that the symptoms could return following withdrawal of oxygen dictates that the patient be transported by ambulance to an emergency medical facility. Dental therapy should also be delayed. Be aware atrial fibrillation is treated with coumadin in order to prevent embolic strokes from the right atrium. Dental surgery in patients taking coumadin requires special considerations regarding the adjustment of the coumadin dose in order to prevent excessive bleeding following surgery. Recommendations for managing the patient on coumadin are provided in a companion Guide, Common Medical Conditions Encountered in Dental Practice 2nd Edition.
Additional Considerations: If the patient has not been evaluated by a physician for a nonsymptomatic cardiac disrhythm, a referral for a physical should occur promptly. Assuming that the patient is stable (nonsymptomatic), and the medical history indicates that the condition is preexisting with monitoring by the patient’s physician, dental care can proceed with caution. Be aware that drugs that increase heart rate or promote cardiac rhythm instability should be used to the minimum extent necessary to complete the dental procedure. Local anesthetic agents containing epinepherine (1/100,000) should be limited to no more than two to three carpules for a dental visit. Plan dental procedures accordingly and give consideration to using pulse oximetry monitoring and/or supplemental oxygen provided through a nasal cannula (deliver oxygen at approximately 4-6 liters per minute). Although used most frequently for conscious sedation monitoring of patients, pulse oximetry may be of value in monitoring blood oxygenation in otherwise conscious, at risk patients undergoing routine dental procedures accompanied by the administration of local anesthetic agents containing a vasoconstrictor. Pulse oximetry provides a noninvasive means of continuously detecting pulse strength and rate, and oxygen saturation of blood circulating to the fingernail bed. Should the oxygenation of blood, heart rate or pulse strength change, the pulse oximeter identifies these changes either by the digital readout, by a change in the sound pitch for each heartbeat or by a preset alarm. This instrument is extremely easy to use, has only a few medical precautions (inaccuracy with carbon monoxide poisoning and severe anemia) and is very helpful in continuous monitoring of circulatory hemodynamics in medically-compromised patients.
Hypertension:
Cause: Hypertension (high blood pressure) is probably the most common medical condition observed in dental patients. High blood pressure results from elevated resistance to blood flow in the peripheral vascular system either due to loss of elasticity in arteries and arterioles or is related to narrowing of vessel lumens (stenosis). Both of these events occur during the process of atherosclerosis. The primary problem with hypertension is that elevated blood pressure ultimately damages the heart (ventricular hypertrophy that eventually can cause heart failure) or damages the organs that are susceptible to elevated blood pressure (kidney, retina and brain). Furthermore, hypertension places the patient at higher risk for stroke and/or development/progression of atherosclerosis. This is particularly important in diabetes where hypertension places the patient at considerably higher risk for adverse cardiovascular events when compared with nondiabetic patients (Please see the Medical Conditions Encountered in the Dental Practice 2nd Edition Guide). Because hypertension is usually asymptomatic, patients are typically not aware of the condition or choose to ignore it.
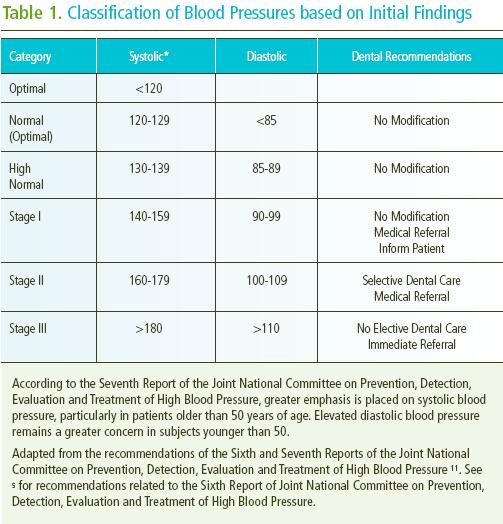
Management: Three types of hypertensive patients can be identified in the dental practice: undiagnosed, noncompliant and medically-treated hypertensive patients5. The noncompliant patient should be strongly encouraged to return to their physician for consultation and to comply with drug regiments prescribed by their physician. Table 1 shows the classification of hypertension based on initial blood pressure measurements. Patients with either stage I or II hypertension should have a follow-up blood pressure measurement within 2 or 1 months, respectively, and if the elevated blood pressure is unchanged, medical referral should occur. Dental care may be provided for stage I and II patients but the amount of epinepherine-containing local anesthetic (1:100,000) administered during a single appointment should be reduced to two carpules but absolutely no more that three carpules should be administered during a dental appointment5. Avoid retraction cord impregnated with epinepherine or epinepherine pellets when taking prosthetic impressions. Patients with stage III hypertension should be referred immediately for medical assessment and treatment and dental treatment should be delayed.
Stage III hypertension can be caused by renal artery stenosis with secondary hypersecretion of renin/angiotensin. Extremely high blood pressures can occur under these circumstances (i.e. 230 mm Hg systolic/140 mm Hg diastolic). Despite this extraordinary blood pressure values, patients may not be aware of the elevated blood pressure. This observation reinforces the need for dentists for dentists to routinely check blood pressure readings particularly in patients with histories of hypertension.
Be aware that patients who are taking antihypertension medications including a non potassium-sparing diuretic may under high stress circumstances develop a cardiac arrhythmia such as atrial flutter or fibrillation. Often these patients are taking potassium supplements to compensate for the potassium loss associated with the use of a diuretic medication. If a patient is not compliant with potassium supplement recommendations, the patient may place himself/herself at risk for a hypokalemic-induced arrhythmia. Under the stress of a dental procedure, the patient with low serum potassium may develop atrial instability that does not resolve with rest, supplemental oxygen or reclined position. A heart rate of 150 beats per minute or greater that is sustained despite rest for longer than 10 minutes should be considered a medical emergency and the patient should be transported to a medical emergency facility for treatment, possibly including cardioversion. In the event of a recalcitrant tachycardia of >150 beats/minute, referral to an emergency clinic should occur regardless of whether the patient feels well enough to leave the dental office. Whenever a medical history includes antihypertension therapy with a non-potassium sparing diuretic and potassium supplements, the dentist should be aware of the possibility that a cardiac arrhythmia can occur simply because of the failure to comply with potassium supplement recommendations.
|