Quality Resource Guide –
Dental Care for Patients with Bleeding Disorders 2nd Edition
www.metdental.com
Page 3
Any patient presenting with an equivocal history
or clinical signs and symptoms suggestive of
an
undiagnosed, or poorly controlled, bleeding disorder
requires further medical evaluation to establish a
diagnosis.
1
While an experienced dental practitioner
may choose to order basic laboratory testing
(Table 2) to assess bleeding risk status (e.g.
activated partial thromboplastin time (aPTT),
prothrombin time (PT), thrombin time (TT), platelet
count), most dentists will refer the patient to their
physician for further evaluation and diagnosis. Once
the specific hematologic impairment is identified, it
must be documented in the patient’s chart.
In spite of obtaining a noncontributory medical
history and noting no abnormalities on clinical
examination, direct observation of excessive
bleeding during or after a dental procedure may
represent the first and only clue for the presence
of a patient’s underlying hematologic impairment.
Suggested Management
Guidelines
E
stablishment of a diagnosis allows the
dentist to develop a plan tailored to address
the dental needs of the individual patient.
Such a plan must not only consider the extent of
surgical therapy needed, but also the patient’s overall
medical status and the clinical experience of the
dentist.
1,3-5
For infrequently encountered scenarios
such as an inherited disorder, a medical consultation
is warranted to determine the patient’s current status
and his/her ability to tolerate the anticipated dental
care in either a general practice or specialist setting.
The dentist should clearly describe in the consult
the anticipated bleeding associated with necessary
dental care (“restore tooth #2 with no anticipated
mucosal incisions or tearing – no, or minimal,
bleeding anticipated”, “simple extraction of two (2)
teeth with primary soft tissue closure following the
procedure – moderate, locally controllable bleeding
anticipated”). In general, a patient determined to
have extensive surgical needs, labile hemostatic
profiles, or the need for treatment modifications not
routinely available in the dental office setting warrant
referral to a practitioner with expertise in managing
such cases (Oral and Maxillofacial Surgeon, Hospital
Dentist or Oral Medicine clinician).
General therapeutic principles recommended when
treating any patient with a hematologic impairment
include:
1. judiciously administering local anesthesia;
2. employing meticulous surgical technique;
3. removing granulation tissue that could mediate
continued bleeding;
4. accomplishing primary soft tissue closure when
possible;
5. using
adjunctive
hemostatic
agents
when
appropriate (see Table 3), and;
6. follow-up contact to ensure no complications.
Postoperative instructions should be clearly
explained and given in written form to the patient
and/or their caregiver to ensure that activities
that may increase the risk of clot disruption
(sucking through a straw, sucking candy, smoking,
rinsing, strenuous activity) are avoided. The use
of any medication that may adversely affect the
underlying hematologic condition, such as aspirin
and NSAIDs, is to be avoided.
1,5,6
Patients with a
hematologic impairment should be scheduled early
in the day, and early in the week, since immediate
complications occur within hours following a
procedure and delayed complications usually occur
within a couple days following a procedure. The
dental practitioner should never adjust the dosage
of any medically prescribed medication (aspirin,
NSAID, warfarin, etc.) intended to affect the
patient’s hemostatic profile. Such adjustments are
under the purview of the managing physician.
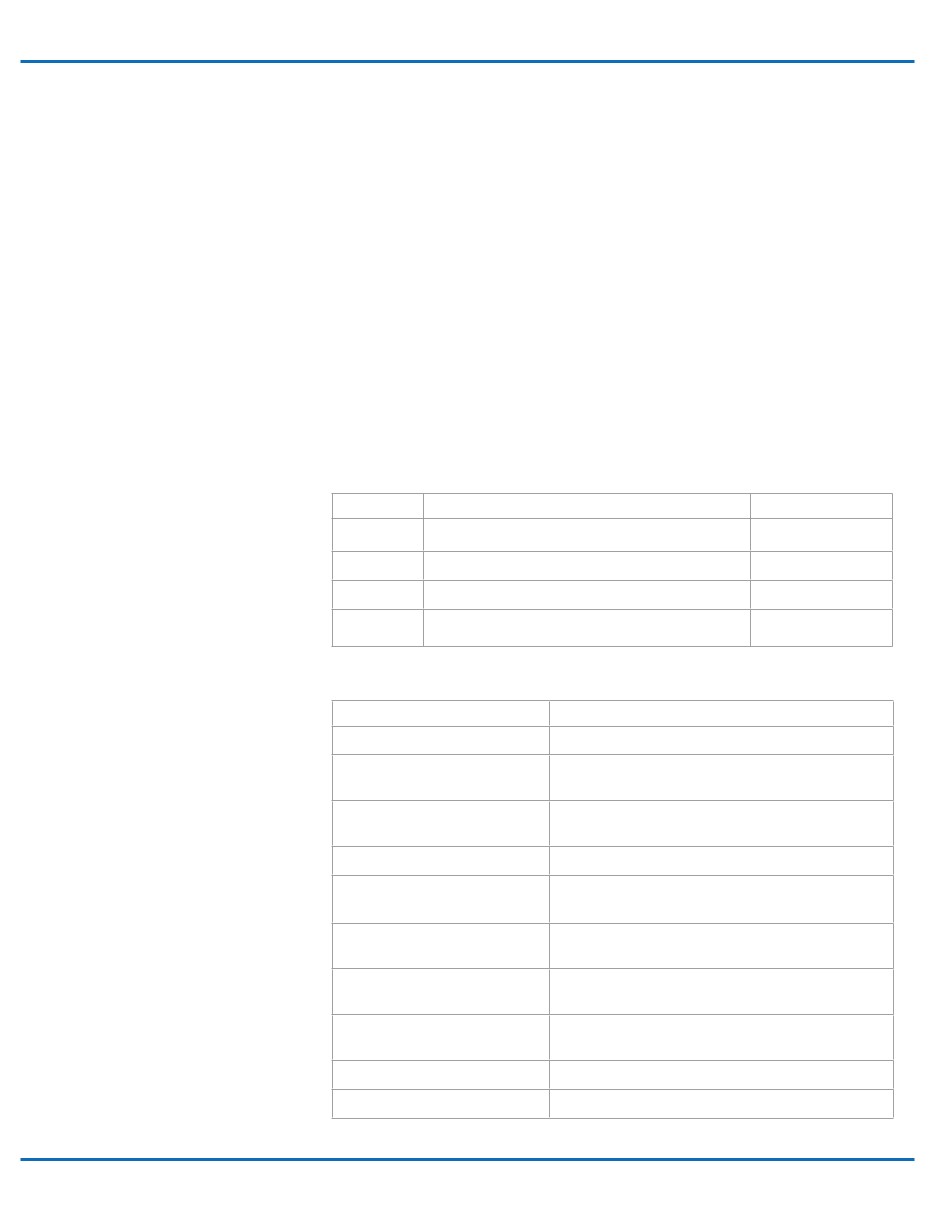
Table 2 - Common Laboratory Tests to Assess Hemostasis
Test
Purpose
Normal Range
aPTT
Evaluate instrinsic and common pathways of coagulation
25-30 seconds
PT
Evaluate extrinsic and common pathways of coagulation
11-15 seconds
TT
Evaluate the level and function of fibrinogen
9-13 seconds
Platelet count
Measure of number of platelets
140,000-400,000/uL
Table 3 - Adjunctive Hemostatic Agents
Agent
Purpose
Gauze
For direct pressure.
Absorbable gelatin sponge
(Gelfoam
®
)
Serves as a scaffolding to help stabilize clot. Recommend
stabilization with suture or splint.
Chitosan
(HemCon
®
Dental Dressing)
Provides a physical barrier to protect wound bed, dissolves
in 48 hours.
Absorbable collagen (Instat
®
)
Can be cut or shaped, similar benefit as gelatin sponge.
Microfibrillar collagen hemostat
(Avitene™ Flour, Avitene™ Ultrafoam™)
Attracts platelets and triggers aggregation to promote
platelet plug formation.
Absorbable collagen dressing
(CollaTape
®
, CollaPlug
®
CollaCote
®
)
Sutured over the wound or placed under stent.
Resorbable oxidized cellulose
(Surgicel
®
, others)
Swells on contact with blood to increase pressure in socket
to enhance hemostasis.
Topical thrombin (Thrombostat™,
Thrombin-JMI
®
, others)
Topical thrombin should not be used with collagen and
cellulose products due to inactivation from pH alterations.
ε-Aminocaproic acid (Amicar
®
)
A rinse that inhibits plasminogen activation.
Tranexamic acid (Cyklokapron
®
)
A rinse that inhibits plasminogen activation.