Quality Resource Guide –
Clinical Decision-Making for Caries Management in Children 5th Ed.
www.metdental.com
Page 2
procedures and preventive therapies. Conversely,
a child that is caries active may require frequent
diagnostic procedures and preventive therapies.
Factors in Decision Making
Clinical Diagnosis
D
ecisions for when to restore carious
lesions, at least, should include clinical
criteria of visual detection of
a hole
in the enamel, visual identification of shadowing
under the enamel, and/or radiographic recognition
of enlargement of lesions over time. Currently,
the longitudinal evaluation of lesion progression
(increased dimension/cavitation of a white spot
lesion or presence of a new lesion) at recall visits
are the best method to determine lesion activity and
progression.
Along with other information, such as
caries risk assessment, the likelihood of a patient
returning for periodic recalls and compliance with
preventive therapy, a carious lesion may require
intensive preventive therapy or restoration, whereas
non-active or arrested lesions may require no
therapy. Such patient-and tooth-specific evaluations
of caries diagnosis and progression has acquired the
term of “active surveillance” where there is careful
monitoring of caries progression and the preventive
program, instead of definitive decisions regarding
the treatment of a lesion at the first sign of disease.
A positive outcome of dental care should be that a
carious lesion shows no evidence of progression at
a periodic recall.
Caries Risk Assessment
T
he goal of caries risk assessment in
dentistry is to deliver preventive and
restorative care specific to an individual
patient. An obstacle in current caries risk
assessment is that few studies so far have attempted
to determine how the application of risk indicators in
dental practice affects dental health outcomes.
The best caries risk indicators are the presence
of caries and the longitudinal evaluation of lesion
progression; however, in pre-school children these
indicators are not particularly useful since it is
important to determine caries risk before disease is
manifest. Other caries risk indicators that have shown
promise in children are: the the level of
mutans
streptococci
in the child; whether the mother/
caregiver has active caries, the socioeconomic
status of the family, and whether the child consumes
sugar at high frequency (see Table 1 for a list of
caries risk indicators).
Besides determining caries risk at initiation
of therapy, ongoing reassessment of a child’s
caries risk at recall visits allows for refinement
of decisions. If at a recall visit, existing lesions
have not progressed and new lesions are not
detected, caries risk may be considered to have
decreased. If there are increased numbers of new
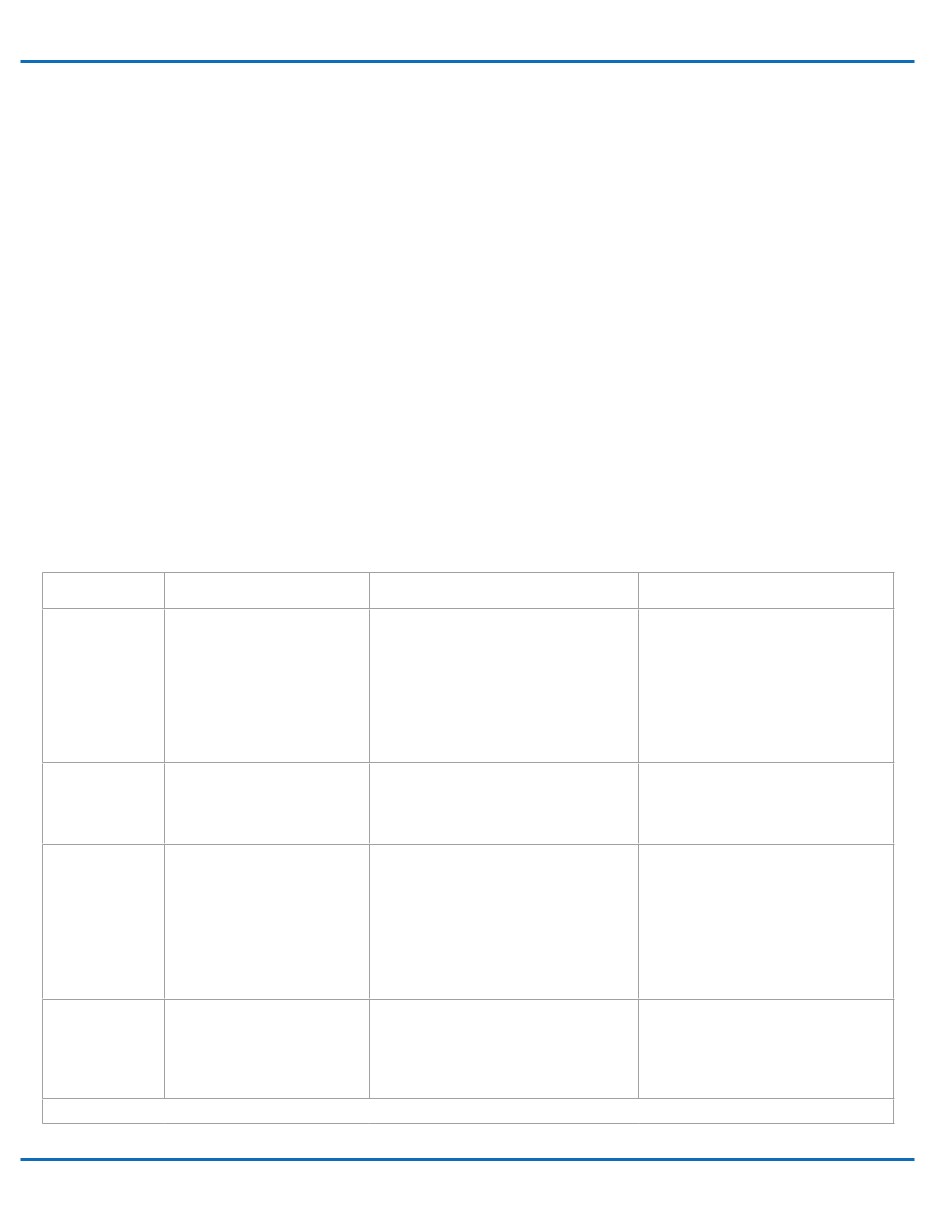
Table 1 - Possible diagnostic procedures, preventive and restorative therapy in primary teeth based on a child’s caries risk assessment.
Low Risk
Moderate Risk
High Risk
Caries Risk
Indicators
• child has no caries
• no new lesions in 1 year
• no white spot lesions
• low titers of MS*
• high SES**
• child has 1 or more lesions
• 1 or more lesions/year
• infrequent white spot lesions
• moderate titers of MS
• middle SES
• child has 1 or more proximal lesions
• more than 2 new lesions/year
• numerous white spot lesions
• high titers of MS
• Mother/caregiver has active caries
• low SES
• appliances in mouth
• high frequency sugar consumption
Diagnostic
Procedures
• examination interval 12 months
• radiograph interval 24 months
• baseline MS** evaluation
• examination interval 6 months
• radiograph interval 12 months
• baseline MS evaluation
• examination interval 3 months
• radiograph interval 6 months
• baseline and follow up MS testing
• diet analysis
Preventive
Therapy
• Brushing with F toothpaste
twice daily
• Brushing with F toothpaste twice daily
• systemic fluoride supplements***
•
professional topical fluorides tx every
6 months
• sealants
• Brushing with F toothpaste twice daily
• systemic fluoride supplements***
• professional topical fluoride tx every
3 months
• sealants
• brushing with high potency F gel
(over age 6)
• dietary counseling
Restorative
Therapy
• None
• active surveillance of white spot lesions
• active surveillance of
enamel proximal
lesions
• restoration of progressing lesions
• restoration of cavitated lesions
• active surveillance white spot lesions
• restoration of enamel proximal lesions
• restoration of progressing lesions
• restoration of cavitated lesions
* MS = mutans streptococci
** SES = socioeconomic setting
*** Age and water supply considerations