Page 7
Quality Resource Guide -
Minimally Traumatic Surgical Extractions in General Practice 2nd Edition
www.metdental.com
they rely on piezoelectric and laser energy, rather
than the force of the operator’s hand, to strip the
PDL around the tooth. The tooth or root can then
be lifted easily out of the socket. An example of a
piezoelectric device and its cutting tip are shown in
Figure 10a and b. At this writing, the author is aware
of five different brands of piezos that can be used
for extractions, ranging from $5,000 to $20,000.
Some of them have several different applications
in the dental office, including periodontal scaling,
removing broken endo files, doing endodontic
surgery, removing implants (instead of a trephine
bur), and various osteotomy procedures. Another
device in this category is the Powertome that utilizes
pneumatic energy and sounds like a “jack hammer”.
Blades of the peizo devices and the pneumatic
device are similar.
Extraction “Systems”
A
relatively new
category of devices is meant to
disengage
roots
from
sockets
by
screwing a drill
tightly into the root canal of
a
broken tooth and
utilizing leverage to pull on the drill. An example of
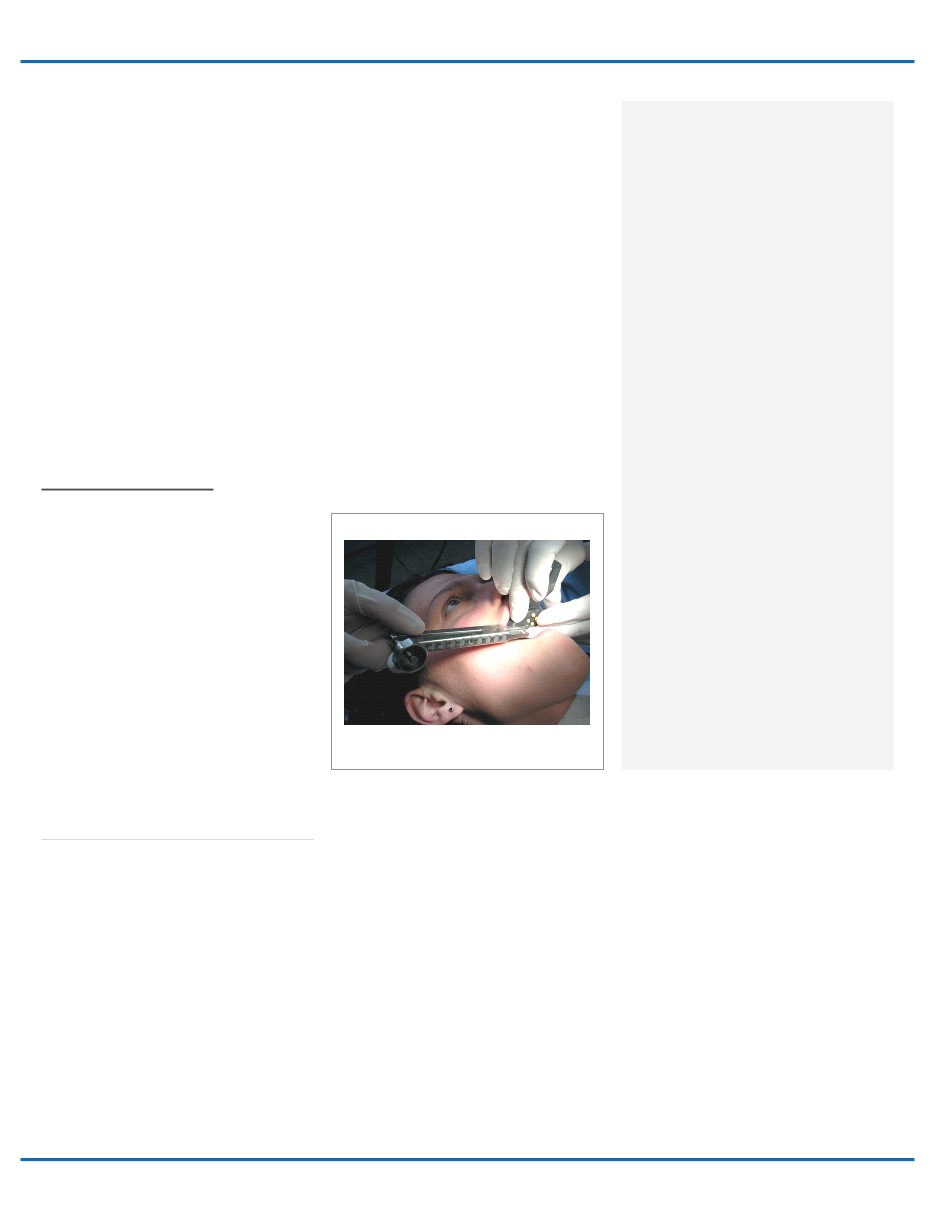
this type of device is shown in Figure 11. First, a
periotome severs the gingival attachments. Then
the drill, which is engaged into the root canal, is
connected to a leverage apparatus that pulls on
the root with sufficient traction to stretch and sever
the PDL. It is truly “atraumatic” in that adjacent
bone is not compromised in any way.
Even in
those infrequent situations where the root cracks
during insertion of the drill, the tooth typically splits
lengthwise and a luxator can usually take the pieces
out of the socket. Examples of devices are the
Easy X-Trac System, Benex/Messinger System, and
Sapian Root Remover System.
Advantages of all these extraction systems include:
1) no bone is removed around the root; 2) the
device does not violate the soft tissue around the
tooth; 3) they are gentle and atraumatic from the
patient’s perspective, and; 4) they are ideal for
creating sites for immediate implant placement. The
disadvantages of the devices are: 1) they are not as
good for molars as they are for single- rooted teeth
(the clinician usually needs to section a posterior
tooth before using these instruments and they are
somewhat awkward when applied in the posterior
of the mouth); 2) they are costly; 3) they are not as
effective if deep decay is present; and 4) the root can
fracture during the process.
Figure 11
An example of a “tooth extraction system”:
The
Easy X-Trac.
Conclusion
I
n difficult economic times and especially
if the general dentist has expertise in
exodontia, he/she is going to retain more
procedures in the office and refer less. Patients
will be more often opt for extractions instead of
higher-priced treatment plans.
Unfortunately, between 10-20% of extractions
become “surgical” even though initially they
may not have appeared to be that difficult.
This can be a problem for some dentists with
limited experience.
However, even if dental
school training with extractions was restricted,
that does not need to stop clinicians from
using various means to increase their surgical
proficiency.
Courses in “surgical” extractions
are available to help enhance clinicains’ ability,
efficiency, speed, and comfort level. The author
and others offer didactic, model participation,
and even patient partition courses.
There are
numerous surgical texts to enhance surgical
knowledge.
This Guide has reviewed many surgical
principles, and presented some new devices
and techniques that will help the general
dentist perform exodontia more quickly, more
competently, more predictably, and less
traumatically, as required in today’s clinical
environment.
It is an important step towards
reaching your goals with oral surgery.
REFERENCES
1.
Christensen, GJ. Bone regeneration and/
or ridge preservation. Clinician’s Report
2(9):1-2, 2009.
2. Hupp JR, Ellis E, Tucker MR, Contemp.
Oral and Maxillofac Surg. 5th ed p. 296,
Mosby/Elsevier 2008.
3. Ibid. p. 298, Mosby/Elsevier 2008.
4. Ibid. pp. 127-131. Mosby/Elsevier 2008.
5. Ibid. p. 113. Mosby/Elsevier 2008.
6. Leonard, M.
Essential Dental Handbook,
Edwab, R., editor. Chapter 10: Oral Surgery.
PennWell Corp., 2003.
7.
McKenzie WS, Rosenberg M. Iatrogenic
subcutaneous emphysema of dental and
surgical origin: a literature review. J Oral
Maxillofac Surg. 2009 Jun;67(6):1265-8.
8. Rehman KU, Monaghan AM, Tong
JL. Air penetration into the tissues
during oral surgery. Anesth Analg. 2008
Sep;107(3):1085.
9.
Arai I, Aoki T, Yamazaki H, Ota Y, Kaneko
A. Pneumomediastinum and subcutaneous
emphysema after dental extraction detected
incidentally by regular medical checkup: a
case report. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. 2009 Apr;107(4):e33-8.
Epub 2009 Feb 8.
10. Davies DE. Pneumomediastinum after dental
surgery. Anaesth Intensive Care. 2001
Dec;29(6):638-41.
11. Hupp, et al. op. cit.. Mosby/Elsevier 2008.
12. Cavallaro JS, Greenstein G and Tarnow DP.
Clinical pearls for surgical implant dentistry,
Part 3. Dentistry Today. Oct. 2010.
(Peer
reviewed article for CE credit).
14. Cavallaro J, Greenstein G, & Greenstein B.
Extracting teeth in preparation for dental
implants. Dent Today.
Oct. 2014. (Peer
reviewed article for CE credit).
15. Misch, CE
and Perez, HM. Atraumatic
extractions: a biomechanical rationale.
Dentistry Today. August, 2008.