Page 3
Quality Resource Guide -
Minimally Traumatic Surgical Extractions in General Practice 2nd Edition
www.metdental.com
An elevator (such as a #301) is placed horizontally
between two teeth to luxate the
tooth needing
removal, yet the fulcrum for the elevator is the
interseptal bone, not the adjacent tooth. To fulcrum
against the tooth not being extracted can cause
injury to the tooth and periodontium leading to
unnecessary luxation of that tooth, pain, tooth
fracture, and breakage/dislodgement of a prosthetic
crown on the adjacent tooth.
When an elevator is
correctly used, rotation of the instrument can be
clockwise or counter-clockwise - each of these
two directions providing a different force vector for
luxation.
Erupted teeth in an adult have a PDL width in the
range of 1-3 tenths of a millimeter.
6
Older patients
may have an atrophied PDL, or it may be non-
existent with the tooth attached directly to bone
(ankylosis). Ankylosis usually requires that roots
needing removal be drilled out peripherally with a
periotome bur or piezo bone cutting device or by
attrition with a round bur.
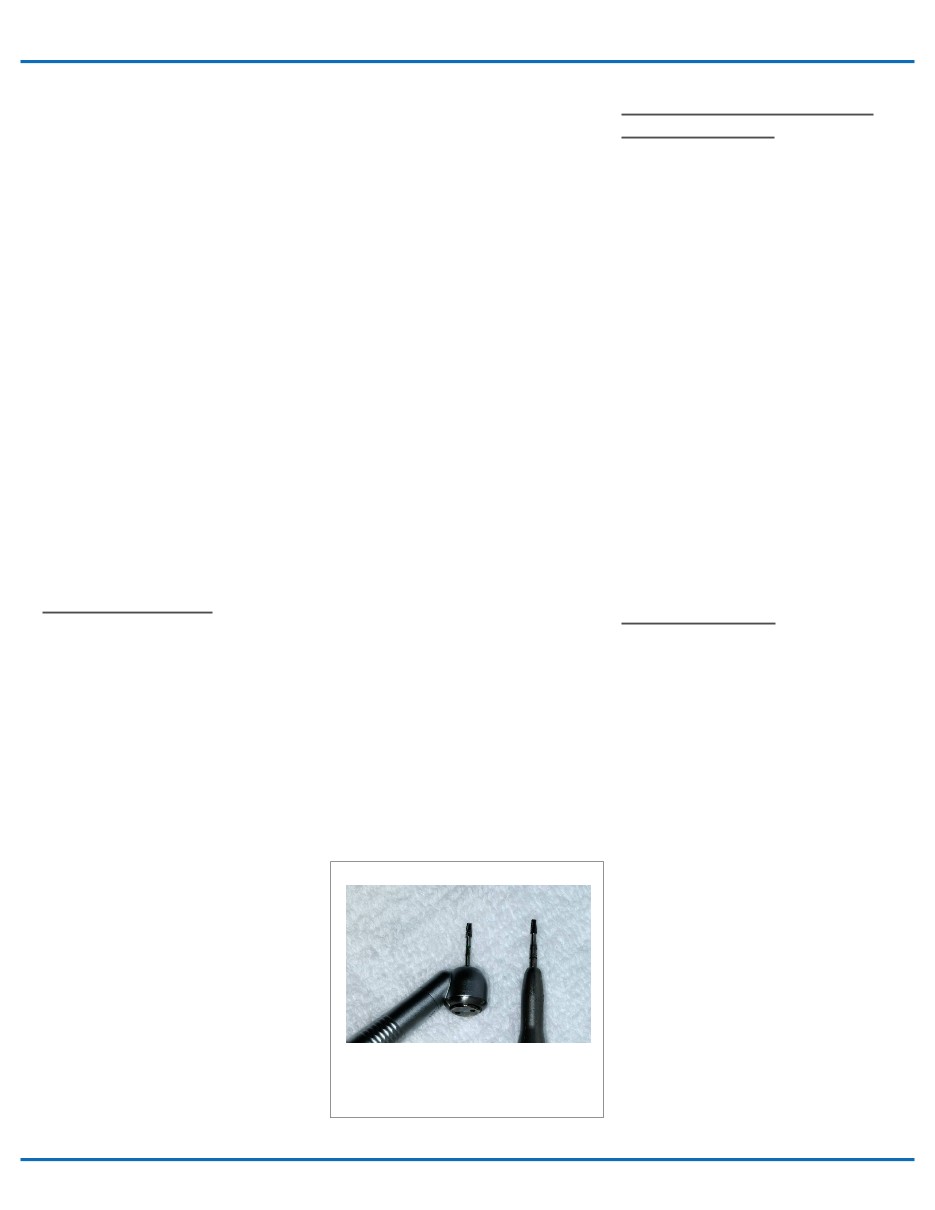
Handpiece Selection
C
hoosing the right handpiece is important when
preparing for surgical extractions. Options for
handpieces include either a straight handpiece
(air turbine or electric) or a “surgical” highspeed
handpiece. Both types of handpieces (Figure
1) are designed so they do not blow air into the
surgical field. When air is forced into soft tissue
during surgery, it creates the possibility of air
emphysema into fascial spaces. This complication
is not limited to oral surgery procedures as the
dental literature also includes many case reports
occurring during restorative procedures or by the
patient blowing air– usually when the soft tissue
attachment around a tooth is violated.
7-10
Air emphysema is manifest by sudden
subcutaneous swelling of soft tissue in the vicinity
of the drilling. It can affect tissue overlying the
mandible or maxilla - and/or extending more
deeply into the infraorbital area, the neck,
and even to the mediastinum. Oral organisms
accompanying the air can potentially cause life-
threatening infections. Should emphysema occur,
a consultation with a specialist is recommended.
Treatment, depending on severity, generally
consists of a clinical evaluation, cone-beam
CT imaging, and appropriate follow-up care
including antibiotic therapy, an anti-inflammatory
medication, and possibly hospitalization.
All drilling of teeth and bone with a handpiece
should be accompanied by irrigation to prevent
overheating and flush away debris. As mentioned
above, the irrigation medium should not be
mixed with air (air-water spray). Sterile saline is
recommended and non-disinfected water coming
through biofilm-laden dental unit tubing is not.
Water is typically delivered through the handpiece
when using a highspeed drill. With a straight
handpiece, irrigation can be delivered separately
by way of a bulb syringe, 12 cc Monoject syringe,
20-30 cc syringe with an irrigation needle, or
from a IV bag with water pumped through tubing
attached to the handpiece.
Complications leading to an untoward experience
during tooth extraction should be infrequent.
If “exceptions” happen routinely, there is the
probability that the dentist is operating outside his/
her range of ability, and thus, outside the standard
of care. One good subjective criterion to use as a
guide during patient case selection is the dentists’
“comfort zone”. If the dentist does not feel right
about starting a case, it should be referred. On
the other hand, clinicians should keep learning
and broadening their expertise throughout their
professional career so that over time, their comfort
level expands.
Care Near Vital Structures and
Inaccessible Areas
Good visibility and careful technique are especially
necessary when a surgical procedure takes place
in close proximity
to vital structures, such as
the mandibular canal (inferior alveolar
nerve),
mental
foramen, lingual nerve, floor of the
mouth
(including the lingual artery), infratemporal space,
the maxillary sinus, facial artery/anterior facial
vein, and the greater palatine artery. Whenever
a surgery procedure approximates these areas
or structures, significant care must be exercised.
If one tries to curette out an abscess apical to
a lower premolar, the mental nerve could be
injured. Excessively long buccal releasing incisions
between the mandibular first and second molars
could approximate the region of the facial artery
and/or anterior facial vein. Manipulation of palatal
tissue lingual to the maxillary second molar could
endanger the greater palatine artery. Inadvertently
letting a straight elevator slip into the floor of the
mouth could puncture the lingual artery.
Bleeding Problems
Bleeding is expected with oral surgery, but
occasionally it can become serious and even life-
threatening. As mentioned previously, the clinician
should avoid actions that could compromise the
lingual artery or facial artery/anterior facial vein.
Incisions near the greater palatine arteries can
lead to difficult-to-control spurting of blood from
the palate. Drilling bone will sometimes expose
a nutrient canals (small blood vessels in bone),
also causing spurting. In the latter case, bleeding
can usually be managed by burnishing adjacent
bone into the bleeding orifice or by pressing a
small amount of bone wax or bone graft into that
spot.
If there is profuse bleeding from a socket,
the clinician can use non-absorbable Iodoform
cotton gauze as a temporary tamponade (leaving it
in place for several days before removing it) along
with the normal 2 X 2 gauze over the socket with
biting pressure. If a dentist does extractions he/she
should use one or more hemostatic local measure,
such as Gelfoam™ hemostatic gauze, Colla-Plug™,
additional sutures, silver nitrate sticks, etc.
Figure 1
Examples of surgical high-speed handpiece (left)
and surgical electric straight handpiece (right).
Both
are engaging a 702 surgical bur, and
both types of
handpieces are acceptable for exodontia.