Quality Resource Guide –
Oral Ulcerative and Vesiculobullous Diseases Part 2 - 4th Edition
www.metdental.com
Page 6
The striae, although occurring typically in
asymmetric pattern on the buccal mucosa
bilaterally, may also be noted on the tongue and
less commonly on the gingival mucosa and the
lips. Almost any mucosal tissue
may
demonstrate
manifestations
of lichen planus. This form (reticular)
generally presents with minimal clinical symptoms
and is often an incidental discovery.
The plaque form of lichen planus (Figure 6)
tends to resemble leukoplakia clinically but has
a multifocal, generally bilateral distribution. Such
plaques generally range from slightly elevated to
smooth and flat. The primary sites for this variant
are the dorsum of the tongue and the buccal
mucosa.
The erythematous or atrophic form of lichen
planus (Figure 7) appears as red
patches with
very fine white striae at the periphery. It may
be seen in conjunction with reticular or erosive
variants. The proportion of keratinized areas to
atrophic areas varies from one area to another.
The attached gingiva, commonly involved in
this form of lichen planus, exhibits a patchy
distribution, often in four quadrants, with
labial /buccal sites more commonly affected
versus palatal and lingual areas. Patients may
complain of burning, sensitivity, and generalized
discomfort.
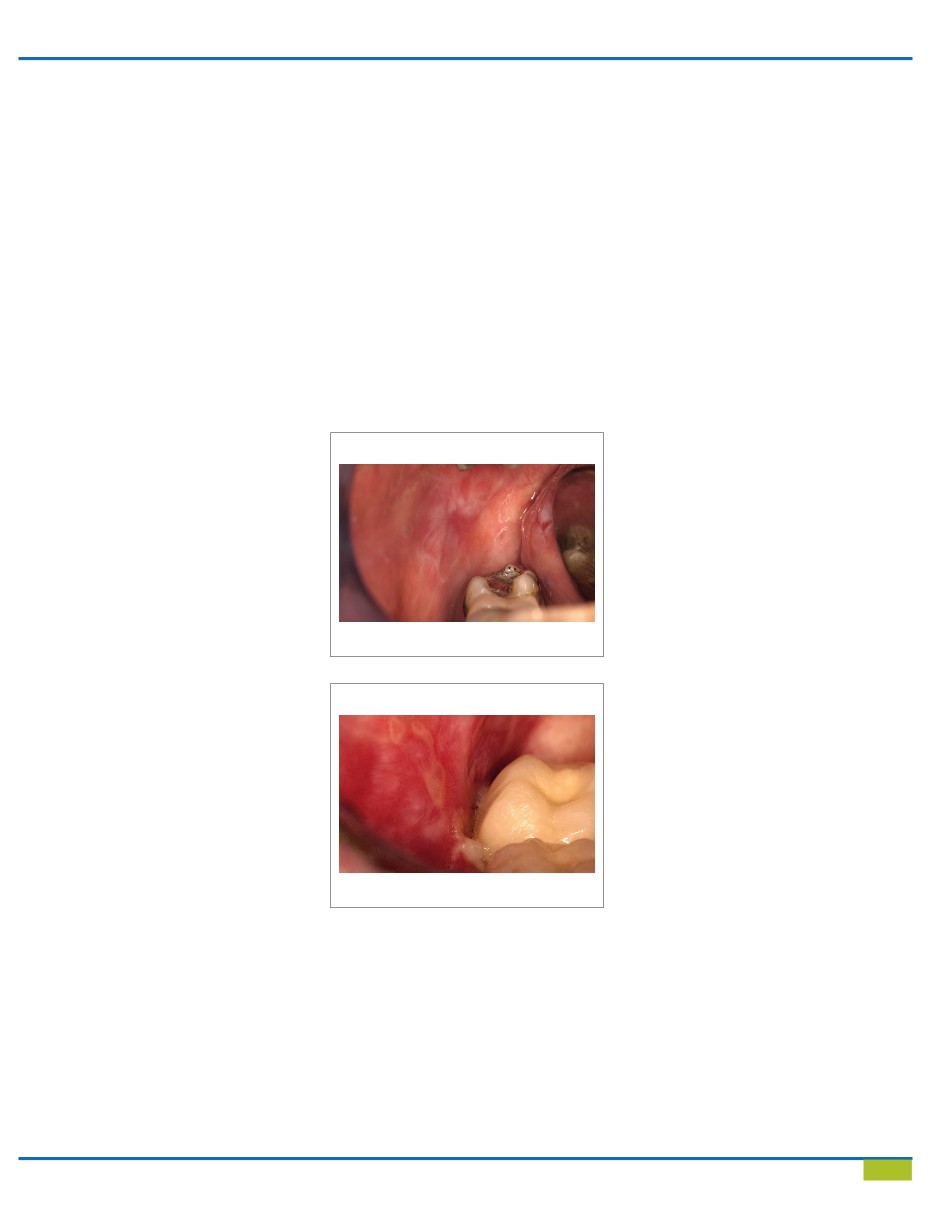
In
the
erosive
form
of
lichen
planus
(Figure 8) the
central
area
of
the
lesion
is
ulcerated. A well-defined fibrinous plaque
or
pseudomembrane covers the ulcer. The process
demonstrates changing patterns of
involvement
noted
from
week to week.
Careful examination usually demonstrates
keratotic striae, peripheral to the site of erosion,
and erythema.
A rarely encountered form
of
lichen
planus
is
the bullous variant. The bullae
range
from
a
few millimeters to
centimeters
in
diameter.
Such bullae are generally short lived and upon
rupturing, leave a painful ulcer. Lesions are
usually seen on the buccal mucosa, especially in
the
posterior
and
inferior
regions
adjacent to
the
second
and
third
molars.
Lesions
are less
common on the tongue, gingiva, and inner aspect
of the lips. Reticular or striated keratotic areas
should
be
seen
elsewhere in the oral cavity with
this variant of lichen planus.
On the skin, lichen planus is characterized by the
presence of small, violaceous, polygonal, flat-
topped, pruritic papules on the flexor surfaces.
Other clinical varieties include hypertrophic,
atrophic, bullous, follicular, and linear forms.
Cutaneous lesions have been reported in 20%
to 60% of patients presenting with oral lichen
planus. Although the oral changes are relatively
persistent over time, corresponding skin lesions
tend to wax and wane and exhibit a relatively
short natural history (1 to 2 years).
Histopathology
The microscopic criteria for lichen planus include
hyperkeratosis, basal layer vacuolization with
apoptotic keratinocytes, and a lymphocytic
infiltrate at the epithelium-connective tissue
interface. With time, the epithelium undergoes
gradual remodeling, resulting in reduced
thickness and occasionally a saw-tooth rete
ridge pattern. Within the epithelium are increased
numbers of Langerhans cells (as
demonstrated
with
immunohistochemistry),
presumably as
an
antigen
processor
to
the
subjacent
T
lymphocytes.
Discrete eosinophilic ovoid
bodies representing the apoptotic keratinocytes
are noted at the basal zone. These colloid, or
Civatte,
bodies
are
seen in other conditions
such as drug reactions, contact hypersensitivity,
lupus erythematosus, and some nonspecific
inflammatory reaction.
Direct
immunofluorescence
demonstrates
the presence of fibrinogen in
the basement
membrane
zone
in
90%
to
100%
of
cases.
Although immunoglobulins and complement
factors may be found as well, they are far less
common than fibrinogen deposits.
Differential Diagnosis
Other diseases with a multifocal bilateral
presentation should be included in a clinical
differential diagnosis are lichenoid drug reaction,
lupus erythematosus, white sponge nevus, hairy
leukoplakia, cheek chewing, graft-versus-host
disease, and candidiasis. Idiopathic leukoplakia
and squamous cell carcinoma might be
considered when lesions are plaque like. Erosive
or atrophic lichen planus affecting the attached
gingiva
must be differentiated from cicatricial
pemphigoid, chronic lupus erythematosus,
contact hypersensitivity and chronic candidiasis.
Treatment and Prognosis
Although oral lichen planus
cannot
generally
be cured completely after a course of treatment,
some drugs can provide satisfactory control.
Topically applied potent corticosteroids are
the single most useful group of drugs in the
management of lichen planus. The rationale for
their use is their ability to modulate inflammation
and the immune response. Topical application and
local injection of steroids have been successfully
used in controlling but not curing this disease.
In
circumstances
in which symptoms are
severe, systemic steroids may be used for initial
management. The addition of antifungal therapy
Erythematous or Atropic form of Lichen Planus
Figure 7
Erosive form of Lichen Planus
Figure 8