Page 7
Quality Resource Guide –
Management of Malocclusion and Skeletal Problems 3rd Edition
www.metdental.com
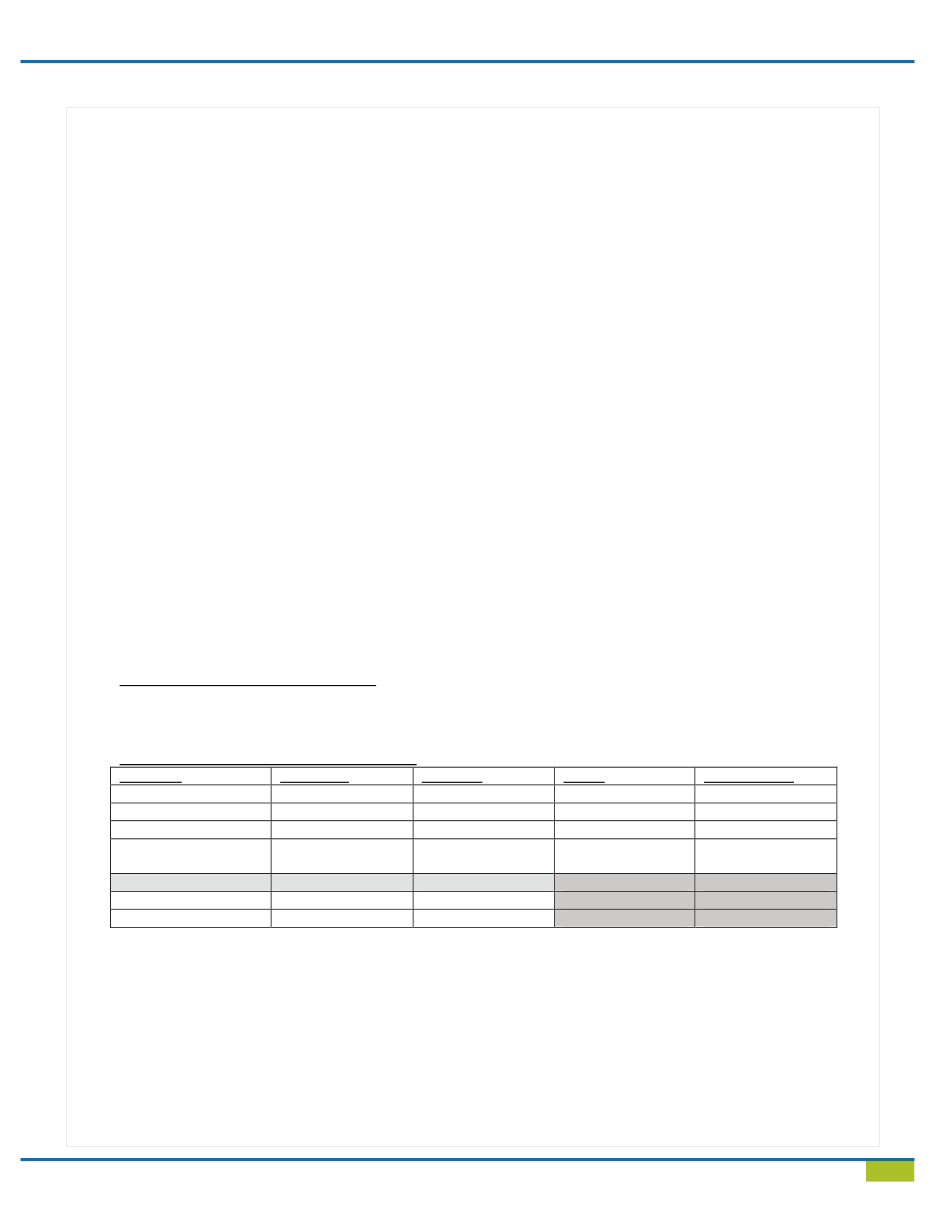
Figure 8 - Orthodontic Diagnosis and Treatment Planning: Patient Evluation Form
Patient Name (last, first)
_____________________________________________________________________________
Date
______________________________________________________________________________________________
Concern(s)_________________________________________________________________________________________
Face Frontal View
_
WNL
WNL
_
Asymmetry
Lips in rest
_
WNL
_
Together Strained [Labial incompetence]
Lower Facial Height [Sn-Me’]
_
WNL
_
Excess
_
Deficient
Max Vertical Height (smile)
_
WNL
_
Vertical Maxillary Excess
Face Profile View
__
Skeletal Class II
_
Skeletal Class III
Abnormal Function(s):
_
Digit sucking [e.g., Thumb]
_
Lip sucking/biting
_
Object sucking/biting
_
Mouth breathing
_
Tongue Thrust Swallow
_
Clenching
_
Grinding/Bruxism
_
Other
Intra-Oral Analysis:
Midline
_
WNL [Upper and lower dental midlines coincide with the facial midline]
_
Upper dental deviated to the
R
_
L
_
_
Lower dental deviated to the
R
_
L
__
Dental Shift
_
Functional shift
Overbite
_
Negative [open bite]
_
WNL [0-30%]
_
Moderate
_
Severe [almost 100%]
Overjet
_
Negative [crossbite]
_
WNL [1-2mm]
_
Moderate [3-5mm]
_
Severe [5+ mm]
Max
_
WNL
_
Crowding
_
Spacing
_
Mild [0-2mm]
_
Moderate [3-5mm]
_
Severe [5+ mm]
Mand
_
WN
L
_
Crowding
_
Spacing
_
Mild [0-2mm]
_
Moderate [3-5mm]
_
Severe [5+ mm]
_
Anterior Crossbite
_
Dental
_
Skeletal [Class III]
_
Functional Shift
_
Posterior Crossbite
R
_
L
__
Dental
_
Functional shift
_
Abnormal tooth position(s) _______________________________________________________________________
Classification of Occlusion/Malocclusion:
_
Normal
_
Class I Mal
_
Class II Div 1 Mal
_
Class II Div 2 Mal
_
Class III Mal
Summary of Problems
[Check ALL that apply]
Condition
WNL/Mild
Moderate
Severe
Not applicable
Overbite
Overjet
Max-Spacing/Crowding
Mand-
Spacing/Crowding
YES
NO
Open bite
Functional shift
Treatment Advice [Check ONE only]:
_
Comprehensive Orthodontic Treatment [COT]
_
COT in conjunction with Growth modification for Skeletal Class II/Skeletal Class III
_
COT in conjunction with Orthognathic Surgery
_
Limited Orthodontic Treatment [1 arch or segmental treatment]: Estimated treatment time______ months
_
No Treatment, Recall Patient in _______month
_______________________________________________________________________________________________
Doctor’s name-- printed and signed
Date