Page 3
Quality Resource Guide –
Management of Malocclusion and Skeletal Problems 3rd Edition
www.metdental.com
arch and 2mm per quadrant in the mandibular
arch as the “leeway space”. Normally, this space
will be lost after exfoliation of the primary teeth
due to mesial migration of the permanent molars.
However, if properly managed, this space can be
used to resolve situations of borderline crowding
.
It
is also important to look at radiographs
when evaluating spacing or crowding.
If teeth
are impacted or at risk for impaction, due to
insufficient space for eruption, the condition
is best described as, “crowding” regardless of
clinical presentation (open contacts).
F. Occlusal Interferences/Mandibular
Functional Shifts
The dentist should describe tooth misalignment
using standardized terminology. A description
should include the tooth or group of teeth, the
type of problem, direction and magnitude of
misalignment. In the frontal view one can detect
problems of tooth angulation (mesial-distal tilt)
and vertical position (up or down). In the sagittal
view one can detect problems of inclination
(facial-lingual tilt). In the occlusal view, one can
detect rotational problems.
Sample descriptions of misaligned teeth are as
follows:
• #8 is angulated mesially 5°
• #8 is intruded 5 mm
• #8 is rotated 5° distolingually
• #8 is retroclined 5°
Misaligned teeth or groups of teeth may create
interferences in the occlusion. The patient
accommodates by shifting the mandible to avoid
the interferences and establishes an alternative
maximum intercuspation position. Functional
shifts are noted during the clinical evaluation of
the patient.
•
Anterior Shift:
If a patient occludes with a
complete anterior crossbite, the patient may
have a skeletal Class III problem or occlusal
interferences resulting in a forward shift to
the mandible. If the patient can bring his/her
teeth edge to edge, he/she most likely does
not have a skeletal problem (this condition is
often called, “Pseudo Class III”).
•
Lateral Shift:
The dentist should evaluate the
maxillary dental midline and the mandibular
dental midline in the maximum intercuspation
position and in a mouth open position. If the
mandibular midline relationship changes from
when the mandible moves from an open to
a closed position, there is likely a lateral
mandibular functional shift. If the mandibular
midline is off to one side and that is consistent
with the side that appears to be in unilateral
crossbite, it is likely that there is a functional
shift of the mandible (Figure 1).
When evaluating “subdivision” or asymmetrical
malocclusions, the dentist should consider if
the mandibular midline shift correlates with the
malocclusion. A functional mandibular shift may
be a contributing factor to the malocclusion.
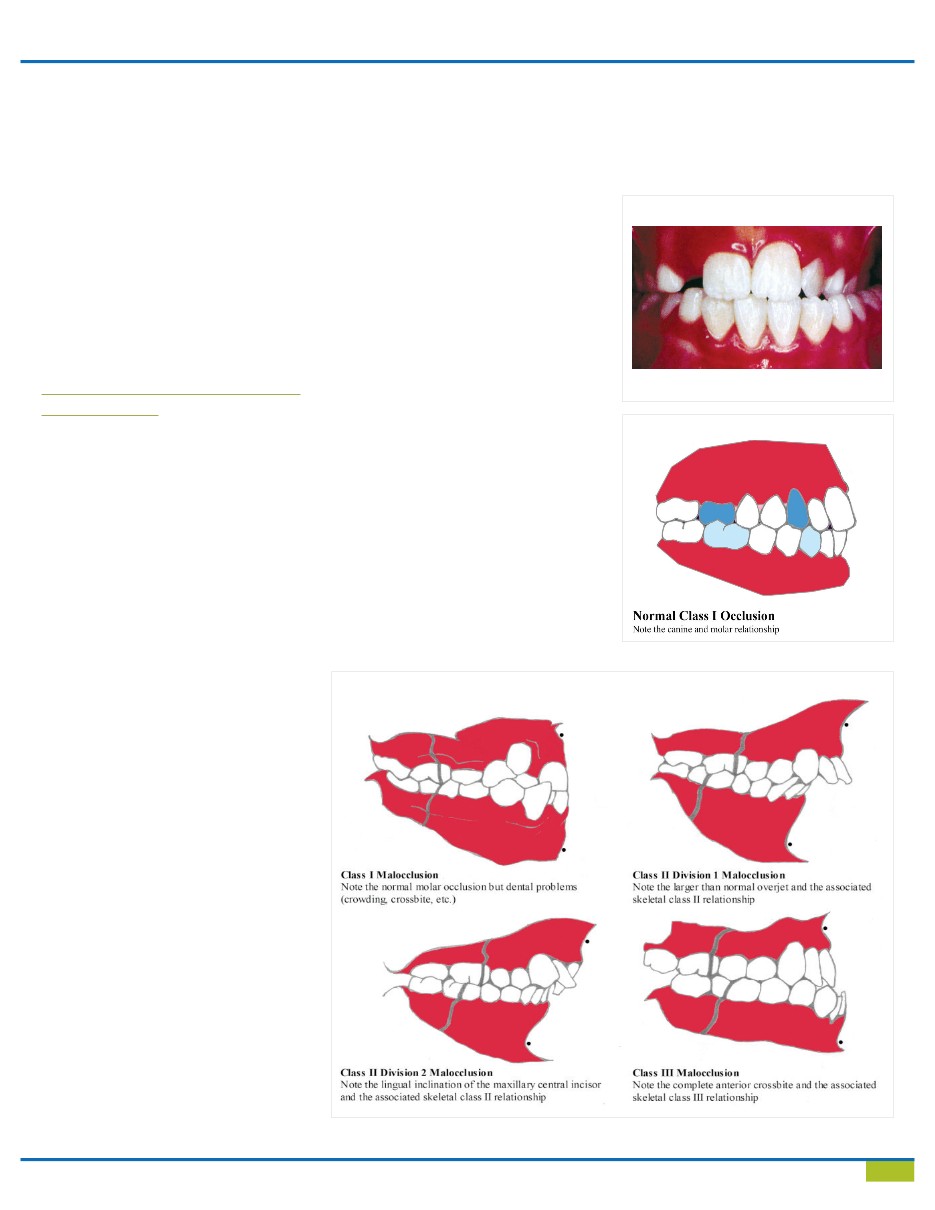
4. Skeletal Conditions
Classification of occlusion is based on the posterior
teeth and canines in maximum intercuspation. In
many clinical situations the occlusion of the molars
alone gives inadequate information. The first step
in the process of accurately analyzing the occlusion
is comfort in recognizing normal occlusion
(Figure 2). Recognizing malocclusion begins with
Angle’s classic descriptions (Figure 3). Angle’s
scheme is useful in identifying problems in the
sagittal [anterior-posterior] plane. The dentist
Figure 1
Left side functional posterior crossbite.
Figure 2
Figure 3