Page 3
Quality Resource Guide –
Managing the Patient with a Worn Dentition 2nd Edition
www.metdental.com
Treatment Planning
W
hen confronted with a complicated
restorative challenge such as worn
dentition, the clinician should return
to the basics of treatment planning, beginning
with the patient interview. What is the patient’s
chief concern? The inability to eat, tooth sensitivity
and poor esthetics are common complaints of the
patient with a worn dentition.
Patients provide important information. They
may relate a history of bruxism, bulimia, or
gastroesophageal reflux disease (GERD); though
individuals with eating disorders might be unwilling
to disclose these problems. Inquiring into dietary
habits may reveal behaviors such as fresh fruit
mulling or the swishing of carbonated beverages,
which can erode tooth surfaces.
2,3
The patient can
be asymptomatic and unaware of the presence
of any of etiologic factors. Referral for medical
evaluation is often indicated in such situations,
which can lead to counseling for any eating
disorders. Many patients will admit to poor dietary
habits that can result in enamel dissolution. Referral
to nutritional counseling will often benefit these
patients.
A thorough review of the medical history, soft
tissue examination, appropriate radiographic
images, periodontal probing, and analysis of the
periodontal tissues and the charting of existing
dental restorations and caries lesions are always
appropriate components of a comprehensive
oral examination. If the dentition appears to be
abnormally worn, the clinician should next evaluate
the interocclusal contacts between maxillary and
mandibular teeth and their contribution to the wear
problem using a diagnostic mounting.
Gypsum casts made from accurate alginate
impressions are sufficient for this purpose.
12
The
casts should be mounted on a semi-adjustable
articulator with accurate facebow and interocclusal
records to properly position them on the articulator.
The facebow (Figure 12) relates the maxillary cast
to the axis of rotation of the patient’s mandibular
condyles and the Frankfort horizontal plane (or
an equivalent third reference point). This allows
the mounted casts to mimic the patient’s occlusal
relationships and mandibular movements. This
mounting can be useful in identifying occlusal
discrepancies and determining how to correct them.
Interocclusal records orient the mandibular cast to
the maxillary cast and are made in centric relation
position (CR). CR is “the relationship of the mandible
to the maxilla when properly aligned condyle/
disc assemblies are in the most anterior superior
position against the eminentia irrespective of tooth
position or vertical dimension.”
13
In contrast, maximum intercuspation (MI) is an
acquired occlusal position where there is maximum
contact between maxillary and mandibular teeth.
CR is selected for mounting the casts because it
is a physiologic, functional, repeatable position.
Methods to guide the patient into CR when making
interocclusal records include: tongue positioning;
14
chin point guidance;
15
bilateral manipulation;
16
the use of a positioning jig;
17
and the use of a leaf
guage.
18,19
After CR is obtained, the interocclusal
record is made using low-resistance media such as
wax, zinc oxide and eugenol, or polyvinylsiloxane
bite registration material.
When occluding casts are mounted in CR, the
initial occlusal contact may be on a single tooth
which prevents the mandible from closing into
MI without first shifting anteriorly and/or laterally.
Over 90% of the population exhibit a discrepancy
between CR and MI.
20-24
These premature contacts
or interferences can be a causative factor for
excessive wear of teeth.
Occlusal Analysis
O
pposing posterior teeth in an ideal occlusion
are located directly over one another so
that occlusal forces load them in an axial
direction (Figures 13 and14). The root structure of
posterior teeth and the orientation of the periodontal
ligaments provide excellent resistance to axial
forces. Maxillary and mandibular anterior teeth
meet at an angle (Figure 13) causing the maxillary
anterior teeth to be loaded in a transverse direction.
Consequently, anterior teeth cannot withstand
heavy occlusal forces.
The position of the anterior teeth forward of the
muscles of mastication and the TMJ (a fulcrum)
creates a class III lever (Figure 15). In this
configuration, the greatest occlusal forces occur on
the teeth nearest the fulcrum. Therefore, occlusal
forces on anterior teeth are low compared to
posterior teeth.
In addition, anterior teeth utilize
proprioceptive indicators to prevent overloading.
25,26
Figures 13 and 14
Anterior teeth are not positioned to take the force of closure of the mandible.
The posterior teeth
will take the force of mandibular closure down the long axis of the individual teeth.
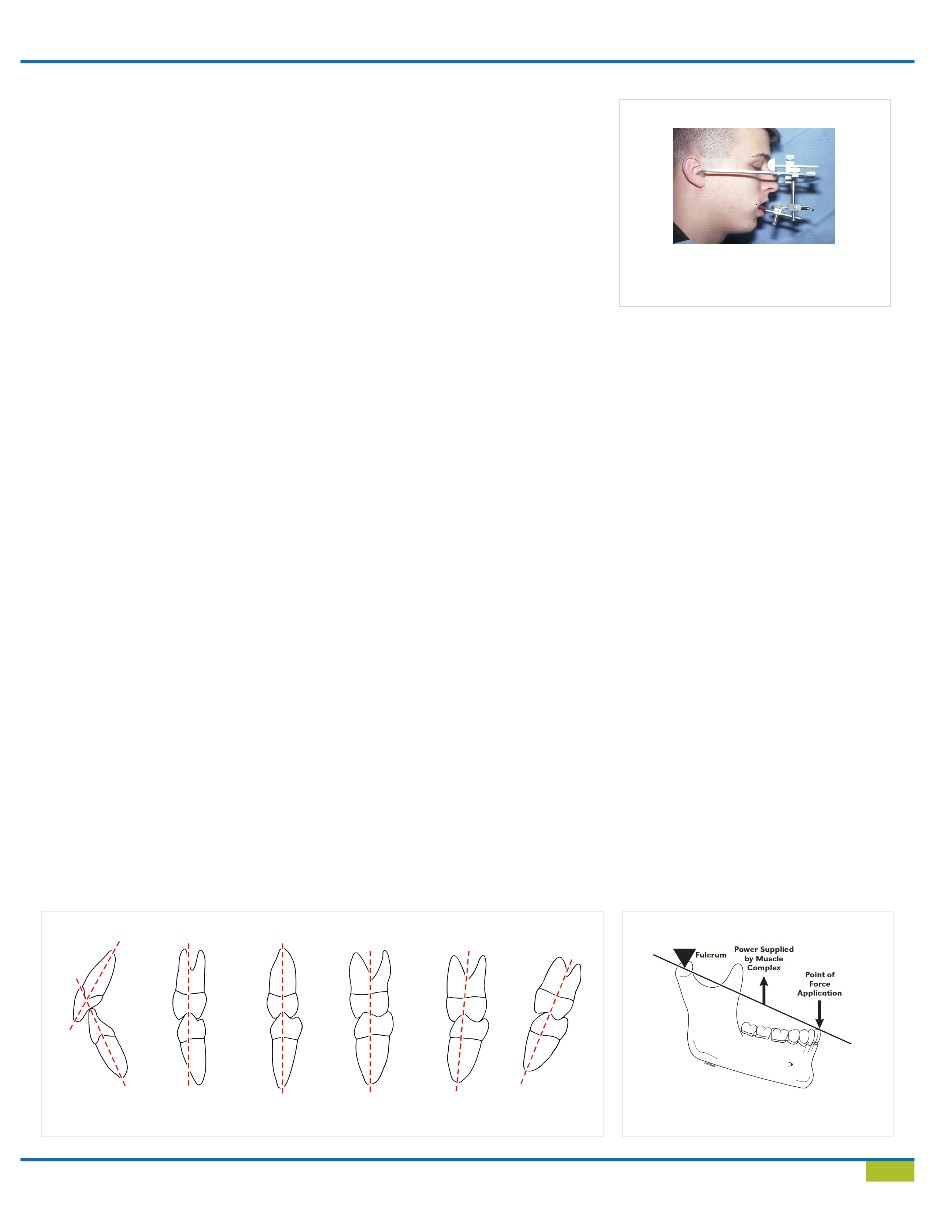
Figure 12
The use of the facebow will relate the maxil-
lary cast to the axis of rotation, the Frankfort
horizontal plane and the plane of occlusion.
Figure 15
The ideal occlusal model will demonstrate
a class III lever.