Page 2
Quality Resource Guide –
Managing the Patient with a Worn Dentition 2nd Edition
www.metdental.com
of stomach contents will normally be greater in the
anterior region of the mouth due to the projectile
vomitus and tongue position. The tongue will often
cover the mandibular anterior teeth protecting
the mandibular anterior teeth,
allowing greater
dissolution of the maxillary anterior teeth, especially
on the lingual surfaces.
5, 6,7,8,9
The use of commercial soft drinks and sports
drinks can also add to the dissolution of enamel. An
analysis of the pH of the commercial drinks reveals
a low pH with the potential of causing enamel
loss.
10,11
Abrahamsen refers to the problem with
commercial drinks as “Coke-Swishing” and states
that the loss of enamel is more prominent in the
posterior of the mouth because of tongue position.
Cupping or cratering is present with the soft drink
erosion and will present sharp enamel edges.
2
Abfraction lesions are wedge-shaped cervical
defects attributed to tooth flexure during abnormal
occlusal loading. The worn dentition is often due to
a combination of attrition, erosion and abfraction.
1-3
The clinician must identify and eliminate all etiologic
factors, before restoring the dentition to proper form
and function.
We often discover that a patient will demonstrate
tooth wear that is a combination of erosion,
abrasion and attrition. Figure 8
shows a patient
with significant tooth structure loss. He had been
diagnosed with gastric reflux problems and was
able to communicate the issue.
Loss of tooth
structure was much greater on the patient’s right
side than his left.
The patient stated he would have reflux episodes at
night, and the taste would drive him to immediately
brush his teeth. He was able to demonstrate that
he would vigorously brush his right side, but barely
touch his left side. Erosion combined with abrasion
as he brushed his teeth in the presence of gastric
acids. He also related to being a right side sleeper,
which allowed gastric contents to concentrate in
the right side vestibule, creating greater erosion.
Figure 10 shows a patient in a right side working
movement. Tooth to tooth contact and resultant
attrition contributed to the tooth loss on the right
side. The patient demonstrates erosion, abrasion,
and attrition, resulting is heavy loss of tooth
structure.
Figure 11 shows the left side with little
loss of tooth structure in contrast to the right side.
Chemical erosion can be caused by a number of
different agents. The dissolution of tooth enamel
requires an acidic environment. Erosion can begin
at a pH of 5.5.
4
Acid can come from gastric contents
either from gastric reflux or bulimia. Regurgitation
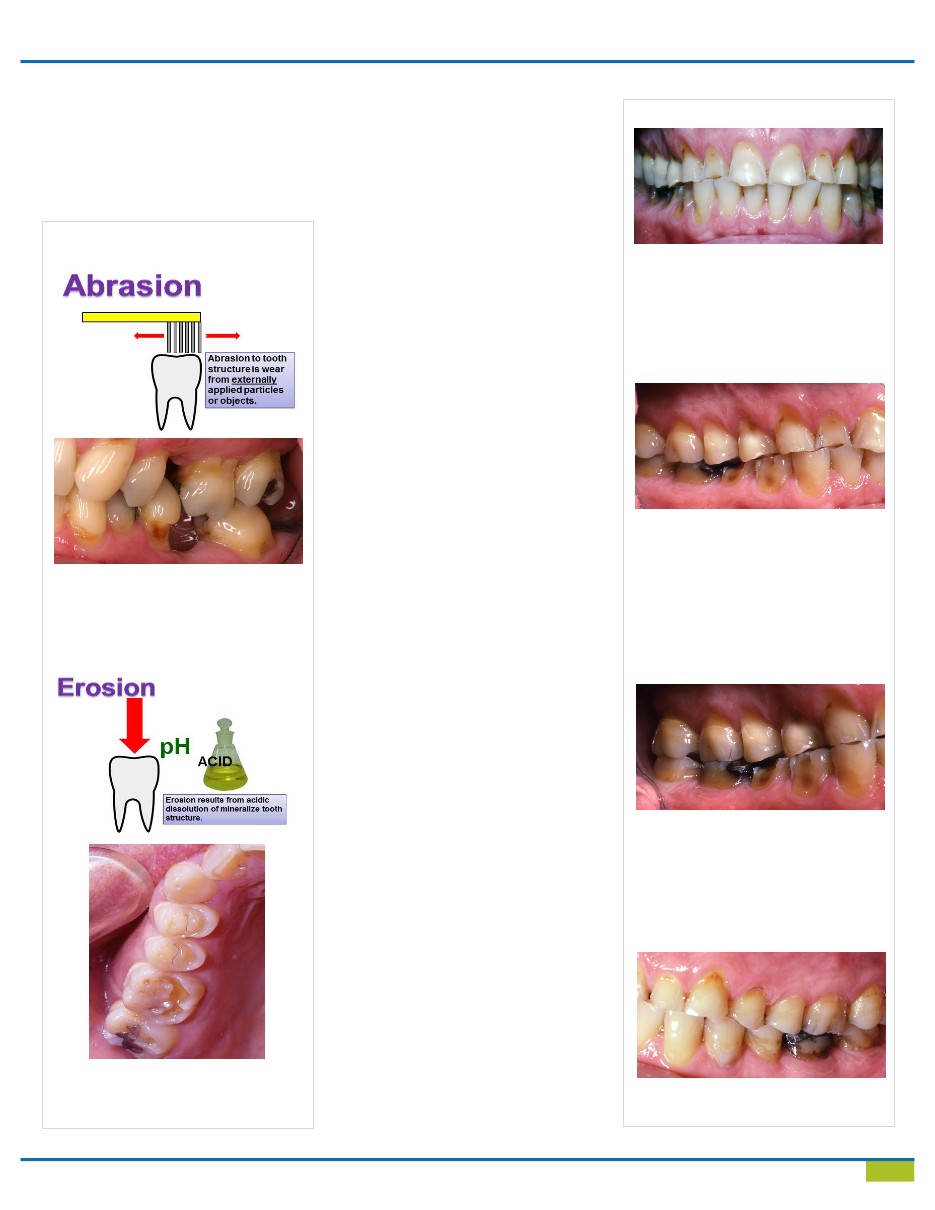
Figures 4 and 5
Abrasion to the facial of tooth #3 and #6.
Probably due to tooth brush use
Figures 6 and 7
Loss of tooth structure on the occlusal
surfaces which do not contact the opposing
arch.
Figure 9
This patient demonstrates significant tooth
structure loss on the facial aspect of the
mandibular molars. Loss is due to both
sleeping position and the pooling of stomach
acid on one side, as well as the use of a
toothbrush to vigorously brush the right side
when stomach acid is present.
Figure 8
This patient demonstrates wide spread loss
of tooth structure. The mandibular incisors
are not affected as much as the maxillary
and posterior teeth. The tongue will protect
the mandibular incisors from stomach acid.
Figure 10
This photo of right working movement
reveals a balanced occlusion with working,
balancing and protrusive contacts. Tooth
loss is due to attrition combined with ero-
sion and abrasive habits.
Figure 11
The patient’s left side is not as affected by
the erosion and abrasive problems.