|
Periodontal Defects and Regenerative Success
Chronic inflammation can result in destructive changes in the component hard and soft tissues of the periodontium, culminating in loss of supporting alveolar bone and periodontal attachment. Resulting gingival pocket formation can be characterized as suprabony (supracrestal), where the base of the pocket is coronal to crestal bone, or intrabony (subcrestal), where the base of the pocket is apical to crestal bone. Suprabony pockets are typically associated with a horizontal pattern of alveolar bone loss that is not amenable to periodontal regeneration with available regenerative therapies. Intrabony pockets, in contrast, are associated with vertical or angular bony defects that are often responsive to periodontal regeneration.
Intrabony Defects
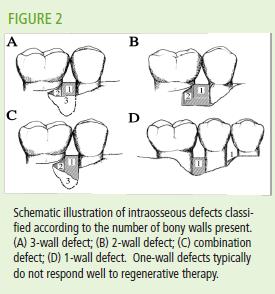
Intrabony defects are commonly described by the number of bony walls (1, 2, or 3 walls) and depth of the defect (measured from the crestal height of bone to the base of the defect). (Figure 2) Periodontal probing and transgingival bone ‘sounding’ can provide important diagnostic information to aid the appropriate selection of regenerative therapy for intrabony defects. Radiographs also provide a valuable tool for selecting defects suitable for regenerative therapy by aiding the estimation of interproximal bone loss; however, radiographic measures generally underestimate bone loss.
Furcation Defects
Loss of periodontal ligament and bone exposing the furcation region of multi-rooted teeth can severely limit plaque control and compromise the tooth prognosis. Therefore, the goal of regenerative treatment is closure of the furcation entrance with hard and soft tissue to improve tooth prognosis and retention. Furcation invasion is most commonly classified according to the degree of horizontal extension within the furcation. For example, furcation invasion is often classified as Class I (incipient loss of bone limited to the furcation flute that does not extend horizontally within the furcation); Class II (variable bone loss that does not extend completely through the furcation; and Class III (bone loss extending completely through the furcation).
Furcation defects are associated with an increased risk of progressive loss of connective tissue attachment, alveolar bone resorption, and tooth mortality. Although early or incipient Class I furcation defects are generally considered maintainable by nonsurgical therapy and effective plaque control, more advanced furcation defects (Class II and III) usually require surgical management for effective inflammatory disease control and tooth retention. Surgery permits access for root debridement, detoxification, and odontoplasty to promote periodontal regeneration. The primary clinical objective in the regenerative treatment of Class II furcation defects is closure of the furcation entrance to the oral environment. Class III furcation defects generally do not respond well to regenerative therapy and are usually treated with surgical debridement or resection.
Gingival Recession Defects
Gingival recession is most commonly a result of chronic inflammation secondary to injury—physical, bacterial, or both. Exposure of the root surface increases the risk of esthetic concerns, root sensitivity, and caries. The most widely used classification system of marginal gingival recession is based on defect characteristics which are correlated with treatment prognosis; namely, the potential to achieve complete root coverage with surgical therapy. The Miller classification system, Class I – IV, is based on the level of the marginal tissue recession in relation to the mucogingival junction, relative tooth position in the arch, and the integrity of the interdental bone and soft tissue morphology (Table 1). Class III and IV recession defects are not amenable to complete root coverage.
|