|
Current Regenerative Therapies
Contemporary therapeutic approaches to
periodontal regeneration include bone replacement grafts, guided tissue
regeneration (GTR), and gingival grafting materials. These regenerative
therapies have been used in combination and in conjunction with agents, such
as biologic mediators, to modify and promote wound healing. Bone Grafting Materials
Historically, the ‘gold standard’ for bone grafting in orthopedics and periodontics has been autogenous bone/bone marrow harvested from the iliac crest. Bone marrow is rich in osteoblasts and progenitor cells that have the potential to form bone (osteogenic) when transplanted into an osseous defect. Nevertheless, multiple clinical considerations have limited the use of autogenous grafts, such as donor site morbidity. Numerous particulate bone grafting materials are commercially available, such as allogeneic bone, xenogeneic bone, calcium phosphate ceramics, bioactive glass, coralline calcium carbonate, among others. Currently, bone allografts are the most widely used grafting materials in periodontal regeneration in the United States. Demineralized freeze-dried bone allograft (DFDBA), or demineralized bone matrix, is allogeneic bone that has undergone extensive mineral removal. DFDBA exhibits the capacity to induce bone formation (osteoinductive) in nonorthotopic sites, such as muscle, due to the exposure of bone morphogenetic proteins. DFDBA has been shown on a histologic level to support periodontal regeneration in humans. With the exception of selected autogenous bone grafts and demineralized bone matrix, most bone replacement grafts are generally considered passive scaffolds providing space maintenance and a framework for cellular migration and tissue formation. Recent attention has focused on the potential for biological mediators to improve wound healing and enhance the clinical benefits of bone replacement grafts. There are two commercially available dental bone grafts with biologic components-- PepGen P-15™ (Dentsply Friadent, Mannheim, Germany) and GEM 21S™ (Osteohealth/Luitpold Pharmaceuticals, Inc., Shirley, NY). PepGen P-15™ is bovine-derived hydroxylapatite (anorganic bone) that contains a short polypeptide chain of 15 amino acids, which is a biomimetic cell binding region of type I collagen normally found in bone. GEM 21S® is a completely synthetic grafting system composed of a purified recombinant human platelet-derived growth factor-BB (rhPDGF-BB) and b-tricalcium phosphate (b-TCP) scaffold. GEM 21S® is the first dental bone grafting material approved by the FDA with a recombinant growth factor. GEM 21S® contains over 1000 times the concentration of platelet-derived growth factor obtainable in current platelet rich plasma preparations (see below). Unlike the particulate bone grafts, Emdogain® (Straumann USA LLC, Andover, MA) is an enamel-matrix derivative comprised of porcine proteins (amelogenins) delivered in a resorbable material (propylene glycol alginate). Emdogain® is classified by the FDA as a device and regulated as a bone grafting material. It is approved for the topical application to root surfaces as an adjunct to surgery.
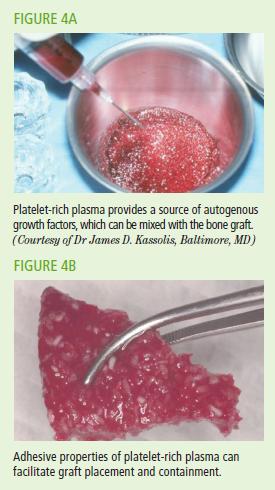
Finally, bone grafts can be combined with growth factors obtained from the serum of a patient. Platelet rich plasma (PRP), collected from centrifugation of serum, provides a source of highly concentrated autogenous platelets containing growth factors, including platelet-derived growth factor and transforming growth factor-b, which are critical for normal healing. When combined with a bone graft, PRP facilitates graft placement and containment. (Figures 4 A-B) PRP has been shown to provide beneficial effects, as reflected in gains in clinical attachment level, when used as an adjunct to periodontal regenerative therapy.
Guided Tissue Regeneration
Guided tissue regeneration (GTR) is a surgical procedure in which a barrier material in the form of semi-permeable membrane is interposed between the mucoperiosteal flap and the bone and tooth surfaces during surgery. Barrier membranes are designed to be biocompatible, cell occlusive, space making, and allow for tissue integration. By impeding epithelial and gingival cell migration onto the root surface and into the intra-osseous defect, barrier membranes promote the selective re-colonization of the periodontal defect with cells supporting the formation of new bone, cementum, and periodontal ligament. Historically, the synthetic membrane expanded-polytetrafluoroethylene (ePTFE) served as the ‘gold standard’ in GTR therapy; however, ePTFE membranes require a second surgical procedure for removal. Currently, the most widely used barrier membranes are made from collagen or polymers, which undergo degradation and, therefore, do not require a second surgical procedure for removal.
Gingival Grafting Materials
The surgical management of exposed roots always involves mobilization of a flap as part of the root coverage procedure. In most instances, the pedicle or coronally positioned flap is combined with a subepithelial connective tissue graft, allogeneic acellular dermal matrix, or GTR barrier membrane. A major advantage of the acellular dermal matrix is the ability to treat multiple recession defects in the same surgical procedure, which may not be practical or possible using autogeous grafts.
|