|
CBCT Technique vs. Panoramic Radiology Technique
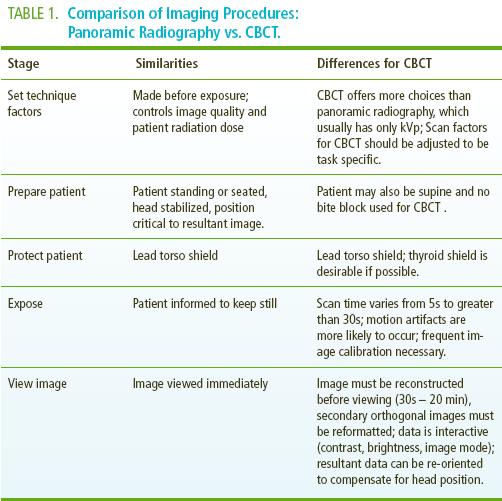
Procedural similarities exist between CBCT and panoramic radiography (Table 1). However, there are also a number of important distinctions between the two techniques, the most important being the greater number of technique parameters available for CBCT imaging.
1) Technical parameters. Two parameters need to be adjusted when performing a CBCT scan; the tube current and the tube voltage. These two factors control the quantity and the quality of the x-ray photons generated by the tube head. They have a direct influence on the quality of the image and the dose of radiation received by the patient. Adjustment of these parameters, if possible, can provide significant dose reduction without compromising the image quality.
In contrast with panoramic radiography, CBCT units also allow additional modifications of scan parameters that may influence image quality and affect patient dose. These include:
A. Field of View (FOV). The tissue volume of the patient’s head exposed during imaging is referred to as the FOV. An adjustable FOV, particularly in large units, is desirable as x-ray exposure should be limited to cover only the region of interest. This provides marked reduction in patient radiation exposure compared to panoramic radiology.
B. Projection data. The total number of basis images comprising the projection data of a single scan may be fixed or variable. This is usually reflected in the selection of scan time. While increasing scan time provides more basis images, and produces "smoother", less grainy images, this is usually accomplished at a higher patient radiation dose.
C. Spatial resolution. While nominal resolution for CBCT units is equipment specific (range: 0.076mm to 0.4mm), the resolution of some CBCT units can be varied at the reconstruction phase using a process of pixel binning (the gathering and combining of information from adjacent regions). This can substantially reduce file size and therefore reconstruction time. Resultant images have reduced resolution but improved image contrast. Higher resolution settings may not be clinically important as patient motion may be the limiting factor in CBCT resolution.
D. Scan arc. Many CBCT imaging systems employ a complete circular (3600) trajectory, however some use a limited, or even a variable, scan arc. A limited or variable arc reduces the scan time and is mechanically easier to perform, however data must be extrapolated to provide a full volumetric dataset. The effect, if any, on diagnostic image quality or radiation dose is currently unreported.
Scan parameter choice should be based on the requirements of the imaging task – a concept referred to as task specific imaging. For example a secondary TMJ scan to determine the degree of translation of the condyle with jaw opening should be performed at the lowest resolution, shortest scan time and reduced FOV. This provides optimal imaging with a nominal radiation dose.
2) Patient Positioning. The patient’s head must be firmly stabilized, whether the they are standing, lying or seated, during the entire scan when obtaining a CBCT image. This reduces the potential for motion during the scan, a significant source of reduced image quality.5 Stabilization can be accomplished using equipment such as chin rests and/or head holders and providing adequate instructions to the patient prior to exposure to remain still during the procedure and to keep the teeth closed either together or on a bite block.
3) Patient Protection. The patient should be draped in a lead torso apron to reduce exposure to scatter radiation during the obtainment of both CBCT and panoramic images. Use of a thyroid collar should be considered when it does not interfere with the area to be imaged as this substantially reduces patient radiation by shielding exposure to the hyoid, esophagus and cervical spine.
4) Exposure Adjustment. Because CBCT exposes the head in one rotational scan, acquisition time is comparable to that of panoramic radiography. However CBCT imaging also incorporates correction and further computational processes on the original projection images. The time for data set reconstruction can be much longer than the scan time and may range from 30 seconds up to several minutes. Image correction necessitates routine calibration of the digital detector, referred to as image calibration, to prevent untoward artifacts affecting image quality.
5) Image Viewing. Unlike panoramic radiography, CBCT units provide a sequential "stacked" set of coronal, sagittal and axial orthogonal images. These images are not inherently easy to interpret. Viewing CBCT images, unlike panoramic images, is performed as an interactive process – windowing and leveling, changing the brightness and contrast, reorienting, rotating or reslicing the volume in all directions may be used by the operator to adapt the final image to his/her diagnostic objectives.
|