|
3. Occlusal Risk Factors [Threshold]
A. Overbite: [100% or if the lower anterior teeth contact palatal tissue]
Overbite is defined as the percentage of vertical overlap of the upper incisors over the lower incisors, and is measured intra-orally or from study casts articulated in the maximum intercuspation position. 100% overbite exists if the maxillary incisors completely overlap the mandibular incisors when the maxilla and mandible are in maximum intercuspation.
B. Overjet: [5+ mm]
Overjet is the distance (in mm) between the facial surface of the mandibular incisors and the maxillary incisors measured at the incisal edge of the most labial tooth. Overjet is measured intra-orally or from study casts articulated in the maximum intercuspation position. Assuming that the maxillary incisors overlap the mandibular incisors, overjet is a positive number. If, however, the mandibular incisors are in front of the maxillary incisors, a condition known as, "anterior crossbite," overjet is expressed as a negative number.
C. Open bite: [Any degree of open bite]
Open bite exists when there is no vertical overlap of the upper teeth over the lower teeth in maximum intercuspation. The millimeter distance of separation between the incisal edges (anterior) or occlusal surfaces (posterior) is the amount of open bite. Open bite can be measured intra-orally or from study casts articulated in the maximum intercuspation position. This condition potentially compromises the patient’s ability to incise or chew food. Any condition that results in masticatory insufficiency is critical for the practitioner to recognize.
D. Dental Crowding: [5+ mm]
The arch perimeter is measured from the mesial of the first molars directly from diagnostic casts. The measurement is broken down to a series of line segments that best describe the idealized arch form. Overlapping contacts are measured (in mm) as areas of crowding. Any condition of crowding above 5 millimeters in a given arch is considered severe. Crowding can also be considered severe if an individual tooth has slipped past the proximal contact more than 2 mm with the adjacent tooth or if it is locked out of the arch.
E. Spacing: [5+ mm]
The arch perimeter is measured from the mesial of the first molars directly from diagnostic casts. The measurement is broken down to a series of line segments that best describe the idealized arch form.
Open contact areas are measured as areas of spacing. When the sum of space is greater than 5 millimeters in a given arch, the condition is considered to be severe. When an arch has both overlapping contacts and open contacts, the dentist should first calculate the overall amount of spacing or crowding in the arch, then itemize areas of particular concern that may affect treatment.
In the transitional dentition, the "leeway space" should be considered when evaluating spacing/crowding. The "leeway space" is the extra space available when the wider primary posterior teeth are exfoliated and replaced by the narrower permanent teeth. As a clinical guideline, 1mm per quadrant should be considered in the maxillary arch and 2mm per quadrant in the mandibular arch as the "leeway space". Normally, this space will be lost after exfoliation of the primary teeth due to mesial migration of the permanent molars. However, if properly managed, this space can be used to resolve situations of borderline crowding.
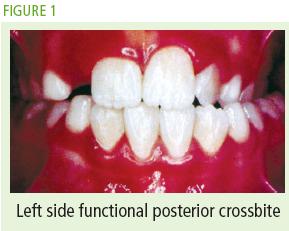
F. Occlusal Interferences / Mandibular Functional Shifts
The dentist should describe tooth misalignment using standardized terminology. A description should include the tooth or group of teeth, the type of problem, direction and magnitude of misalignment. In the frontal view one can detect problems of tooth angulation (mesial-distal tilt) and vertical position (up or down). In the sagittal view one can detect problems of inclination (facial-lingual tilt). In the occlusal view, one can detect rotational problems.
Sample descriptions of misaligned teeth are as follows:
#8 is intruded 5 mm #8 is rotated 5° distolingually #8 is retroclined 5° Misaligned teeth or groups of teeth may create interferences in the occlusion. The patient accommodates by shifting the mandible to avoid the interferences and establishes an alternative maximum intercuspation position. Functional shifts are noted during the clinical evaluation of the patient.
When evaluating "subdivision" or asym metrical malocclusions, the dentist should consider if the mandibular midline shift correlates with the malocclusion. A functional mandibular shift may be a contributing factor to the malocclusion.
|