|
Dental Trauma
Traumatic dental injuries in adolescence are
related frequently to risk taking behaviors that result from motor vehicle
accidents, altercations with peers, or participation in recreational
activities and organized sports. One overarching principle in the successful
clinical management of traumatic dental injuries is to minimize the time
between the injury and the initiation of dental intervention. Not only
does the time factor influence the prognosis for the injury, it is also a
deterrent to future litigation based on claims of abandonment for a patient
of record.
Successful treatment for traumatic dental
injuries in the young permanent dentition also depends on the information
gained through various diagnostic procedures. A determination of the nature
of the accident will provide information not only on the time since the
accident occurred, but also information from medico-legal and insurance
perspectives. Subjective symptoms reported by the patient as to type of
sensitivity or pain may be beneficial in determining the status of pulp
vitality. In addition to visual clinical examination, radiographs are
indicated to determine the extent of any fractures of the crown or root, the
degree of displacement for luxation injuries and any associated alveolar
bone involvement. It also is essential to determine the status of root end
closure since the treatment options often depend on the degree of maturity
of the root apex. Electrical pulp testing is frequently not definitive
immediately following a traumatic dental injury and percussion testing may
be ill-advised as it may further aggravate the traumatic insult to the
tooth.
Following appropriate diagnostic procedures, the
treatment plan for young permanent teeth can be established with the
following goals in mind: to maintain the tooth in the dental arch; to
maintain pulp vitality; to prevent root resorption; and to restore form,
function, and esthetics. For the purposes of this resource guide, the
management of traumatic dental injuries will be categorized as crown
fractures, root fractures, and luxation injuries including avulsion. Crown Fractures
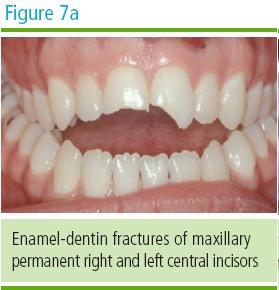
Crown fractures to vital teeth that extend into the dentin are sensitive to touch and temperature changes. In these instances the exposed dentin should be protected with a calcium hydroxide paste prior to bonding the acid-etched composite resin restoration to the enamel (Figure 7A and 7B). Another option is the placement of a composite resin that is directly bonded to the dentin. In those instances in which the fractured portion of the crown has been recovered and is of adequate size, the crown fragment can be reattached to the remaining portion of the tooth using a dentinal bonding agent.
Crown fractures that extend through the enamel
and dentin into the pulp are more complicated from diagnostic and treatment
perspectives. In addition to the diagnostic procedures listed above,
treatment planning decisions for enamel-dentin-pulp fractures also should be
based on pulp vitality status and the degree of root end closure.
In those instances where the pulp is vital and
the apex is closed, the placement of calcium hydroxide followed by an
acid-etched composite resin restoration remains a good option. Dentin bridge
formation beneath the calcium hydroxide dressing can be anticipated as well
as the maintenance of pulp vitality. Another option is the use of mineral
trioxide aggregate (MTA) as the dressing on the exposed pulp, followed by an
acid-etch composite resin restoration. MTA results in the formation of a
denser dentinal bridge than calcium hydroxide; however, the costs associated
with the use of MTA far exceed that of calcium hydroxide. Using a dentin
bonding agent directly over a vital pulp exposure is not supported by the
scientific literature.
For situations where the fracture extends into a
vital pulp with an open apex, the treatment goals are to preserve pulp
vitality, establish a dentinal bridge over the exposure and stimulate
physiologic root end closure. The procedure to accomplish these goals is
known as apexogenesis and is of particular importance in the young
adolescent dentition. This procedure includes the removal of a portion of
the coronal vital pulp tissue. In the more traditional technique, the entire
coronal pulp tissue is amputated leaving the remaining vital radicular pulp
in place. In the more conservative and equally effective Cvek technique,
only a few millimeters of the superficial vital pulp tissues are amputated
at the exposure site using a round diamond bur with high speed cutting and
water spray. Hemorrhage control is followed by the choice of either calcium
hydroxide paste or MTA as the dressing over the vital pulp. The procedure is
completed by the appropriate restoration to restore form and function to the
fractured crown. Dental bonding agents used directly over an exposed vital
pulp should be avoided. Following dentinal bridge formation and root end
closure in asymptomatic teeth, continued follow-up observation is
recommended. If the tooth remains asymptomatic, then no further treatment is
indicated. Endodontic intervention may become necessary if internal root
resorption or periapical pathology become evident radiographically.
Fractures into a non-vital pulp with an open
apex require a technique known as apexification. Since the pulp already is
non-vital, an attempt to induce root end closure is desirable prior to
initiating traditional root canal therapy. This technique involves entering
the canal for mechanical instrumentation and irrigation with sodium
hypochlorite. After drying the canal, a calcium hydroxide- terile water
mixture is delivered into the canal. This material remains in place to
induce a calcific root end closure. Radiographic observation is crucial as
the dressing may need to be changed periodically or if there are any
radiographic signs of internal root resorption. Following the completion of
the root apex, traditional root canal techniques can be performed and an
appropriate restoration placed. For a fractured crown with a non-vital pulp and closed apex, traditional root canal therapy is indicated.
Middle one-third root fractures frequently are
accompanied by displacement of the coronal segment of the fracture. In these
instances, the distance between the stable root portion and the displaced
coronal portion must be reduced with sufficient finger pressure to realign
and approximate the two segments. The tooth should be stabilized with a
semi-rigid, passive wire splint held in place with a small amount of
composite resin material covering the wire over each tooth that is splinted.
Generally, the tooth in question and one tooth on either side of the
root-fractured tooth are sufficient to secure the splint. The splint should
remain in place for 6 to 8 weeks and the tooth should be evaluated
radiographically over this time frame for any adverse developments. In
addition, it is essential for the adolescent to brush the area meticulously
to diminish the ingress of bacterial contamination through the gingival
sulcus. Rinses with 0.2% chlorhexidine gluconate are beneficial.
Fractures in the cervical one-third of the root
are more problematic. They may require endodontic treatment, orthodontic
extrusion, or periodontal crown lengthening for adequate restoration. Often
the treatment of choice is extraction with subsequent replacement of the
missing tooth in an adolescent patient. As the root apices in young
permanent teeth have yet to mature, permanent replacements should be delayed
until tooth development and physical growth have been completed.
Possible temporary replacements may include a
“flipper” partial denture or a prosthetic tooth added to an orthodontic or
retaining-type appliance. A more permanent replacement such a single tooth
implant should be delayed until the completion of the growth potential in
adolescent patients. Of particular note, consideration must be given to the
completion of passive eruption of the permanent teeth prior to placement of
the implant. Even though implant placement in adolescent women over 15 years
of age and adolescent men over 18 years of age has been suggested, it may be
more prudent to delay placement until at least 18 to 19 years based on the
completion of passive eruption.
For additional information related to crown and
root fractures in the permanent dentition, the reader is referred to the
MetLife Quality Resource Guide entitled, Traumatic Injuries and Tooth
Fractures, 2nd Edition. Displaced Teeth
The first principle in the management of a
displaced tooth that remains in the socket is to reposition the tooth into
its normal position. This is followed by the placement of a passive
semi-rigid, composite bonded wire splint for 7 to 10 days. Meticulous home
care is essential and the use of 0.2% chlorhexidine gluconate is beneficial.
Particular note should be taken for any radiographic signs of external root
resorption. If resorption develops or if the tooth becomes symptomatic, root
canal therapy is recommended. For avulsed (exarticulated) teeth the best recommendation is to reinsert the tooth back into the socket as soon as possible. The tooth should be handled carefully by the crown only to avoid additional damage to the PDL tissues that remain on the root surface. If debris is observed on the root or PDL, it should be removed gently with a stream of liquid such as water, milk or Hank’s balanced saline solution. The root or PDL must not be scraped in any manner. Following reinsertion of the tooth back into the socket, the patient should be asked to bite down gently on gauze and transported to the dental office for splint placement.
|