|
Acute Gingival Conditions
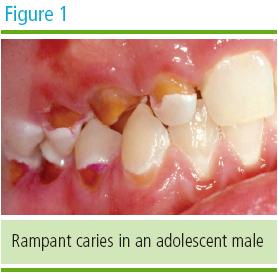
Dental Caries
While caries patterns in children are more
localized to the pits and fissures of young permanent teeth, adolescents
experience more smooth surface lesions, especially in interproximal areas.
The upward incidence in dental caries among adolescents has been attributed
to immature permanent tooth enamel, total increase in susceptible tooth
surfaces, and environmental factors such as independent diet choices, care
seeking and avoidance. (Figure 1) Interventions to interrupt active caries
among adolescent patients should take advantage of the adolescent’s inward
focus on the self. Dental health care providers need to invest sufficient
time and develop enhanced communications with their adolescent patients, on
a one-on-one basis, to increase the likelihood that the patient will become
intrinsically motivated to practice an effective oral health regimen
throughout adulthood, perhaps remaining caries-free.
Daily flossing of the interproximal surfaces of
the teeth combined with tooth brushing using a fluoride containing
toothpaste are essential. In addition, professionally applied topical
fluoride agents and fluoride mouth rinses for home use are beneficial for
those at increased risk. Community water fluoridation has proved to improve
dental health substantially for persons residing in such communities.
An area of increasing concern with devastating
effects on the dentition is methamphetamine abuse and its impact on oral
health. Methamphetamine is a readily available and comparatively inexpensive
illegal drug. According to a national survey published in 2003, the majority
of users are between 18 and 34 years of age; 12.3 million Americans have
tried this substance at least one time. Rampant tooth decay is a common side
effect among addicts, including adolescents. Affected teeth often appear
discolored, decayed, and destroyed beyond repair, frequently requiring
extraction. The 12-hour duration of the drug’s effects contributes to the
multifactorial etiology of this form of rampant decay. These factors include
xerostomia, acidic oral environment, increased craving for carbonated
beverages, increased clenching and grinding of teeth, and lack of attention
to oral hygiene.
Methamphetamine users may exhibit both
behavioral and physiological disturbances. Behavioral components may include
inability to sit still in the dental chair, irritability, excessive talking,
and exaggerated behavior. Observation of these behaviors should alert the
dentist to evaluate several physiological parameters. Methamphetamine may
cause dilated pupils, increased blood pressure, irregular heart beat,
increased respiratory rate, tremors, and convulsions, among others. These
adverse effects must be considered in the choice and administration of local
anesthetics with epinephrine to diminish the possible precipitation of a
dentally related medical emergency from the vasoconstrictor effects of the
epinephrine. Prior to the administration of any local anesthetic agent in a
methamphetamine user, blood pressure should be measured and if high
(systolic > 180 mm of Hg or diastolic > 110 mm of Hg), treatment should be
postponed. Dentists who treat adolescent patients should be alert to possible intraoral signs of methamphetamine use such as a sudden increase in dental caries along with unusual caries patterns that often challenge the skills of the dentist to provide functional esthetic restorations. For example, large facial surface and cervical decay on both maxillary and mandibular anterior teeth, as well as attrition and destructive caries on the posterior dentition provide an entree for questioning the adolescent regarding abuse of methamphetamine.
As patients mature from childhood to
adolescence, increased emphasis should be placed on periodontal health. Both
reversible and irreversible periodontal diseases become more prevalent
during this period. The combined effects of genetics, nutrition, and
hormonal fluctuations all contribute to the increased likelihood for
developing adolescent periodontal diseases. While adolescent patients may be susceptible to a wide spectrum of periodontal diseases, this educational resource guide will highlight some of the more common conditions likely to be encountered by the dental health team.
|