|
Pulp Therapy For Primary Teeth
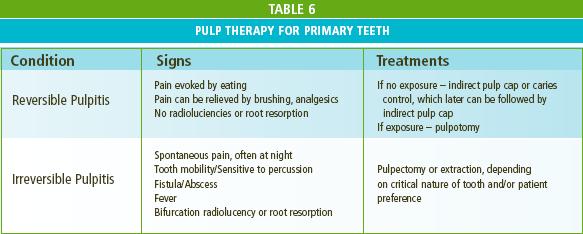
If a child presents with pain from a carious primary tooth, it is critical to determine whether the pulp has reversible or irreversible pulpitis. Those primary teeth with pain evoked by eating, but which diminishes within 1/2 hour and/or shows no signs of infection (Table 6) should be treated to preserve pulp vitality. Recent trends suggest that such teeth have better outcomes if treated initially with a caries control procedure. This is accomplished by excavating gross caries, followed by temporization with a material that covers and seals all exposed dentin. Most often after such treatment the tooth is asymptomatic, and definitive treatment can be performed several weeks later. The definitive treatment for such deep caries in primary teeth often involves careful excavation of the remaining caries trying not to expose the pulp. “Woody dentin” just above the pulp can be left (indirect pulp cap) and covered with a material that seals and stimulates reparative dentin. If excavation results in a pulp exposure, then the vital coronal pulp should be completely and treated with either formocresol, ferric sulfate or Miner trioxide aggregate (MTA). In contrast, if a child presents with spontaneous pain, especially waking the child at night, and other signs of irreversible pulpitis are present, the treatment should be pulpectomy or extraction, depending on the importance of the tooth (i.e., second primary molars that are not near exfoliation) and the desires of the parent.
|